Division of General Medicine, Columbia University Irving Medical Center, New York, New York, USA; Center for Health Services and Outcomes Research, Northwestern University, Chicago, Illinois, USA; Health Economics and Health Technology Assessment, University of Glasgow, Glasgow, United Kingdom.
Division of General Medicine, Columbia University Irving Medical Center, New York, New York, USA.
J Am Coll Cardiol. 2021 Nov 16;78(20):1954-1964. doi: 10.1016/j.jacc.2021.08.065.
Raised low-density lipoprotein cholesterol (LDL-C) in young adulthood (aged 18-39 years) is associated with atherosclerotic cardiovascular disease (ASCVD) later in life. Most young adults with elevated LDL-C do not currently receive lipid-lowering treatment.
This study aimed to estimate the prevalence of elevated LDL-C in ASCVD-free U.S. young adults and the cost-effectiveness of lipid-lowering strategies for raised LDL-C in young adulthood compared with standard care.
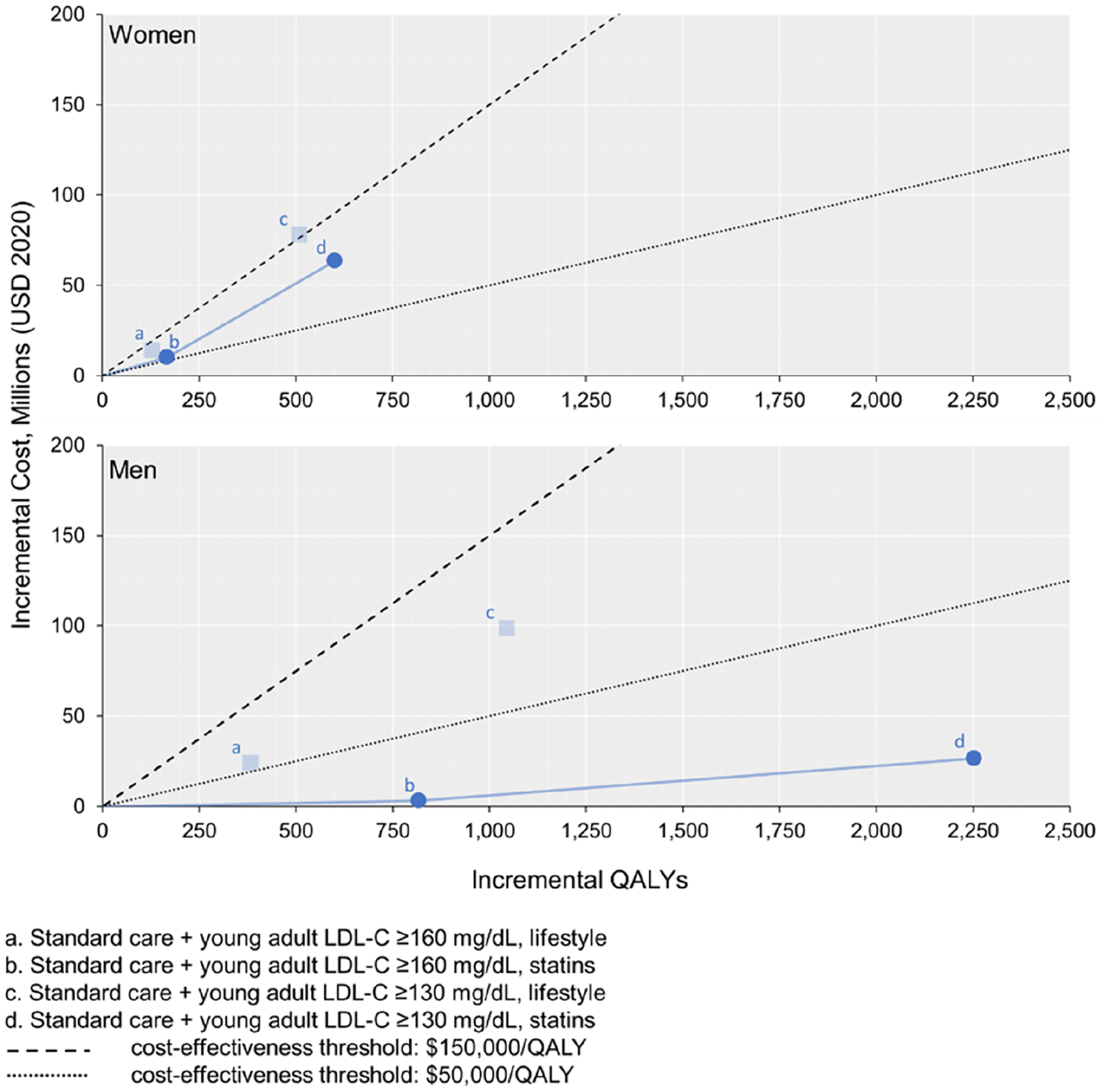
The prevalence of raised LDL-C was examined in the U.S. National Health and Nutrition Examination Survey. The CVD Policy Model projected lifetime quality-adjusted life years (QALYs), health care costs, and incremental cost-effectiveness ratios (ICERs) for lipid-lowering strategies. Standard care was statin treatment for adults aged ≥40 years based on LDL-C, ASCVD risk, or diabetes plus young adults with LDL-C ≥190 mg/dL. Lipid lowering incremental to standard care with moderate-intensity statins or intensive lifestyle interventions was simulated starting when young adult LDL-C was either ≥160 mg/dL or ≥130 mg/dL.
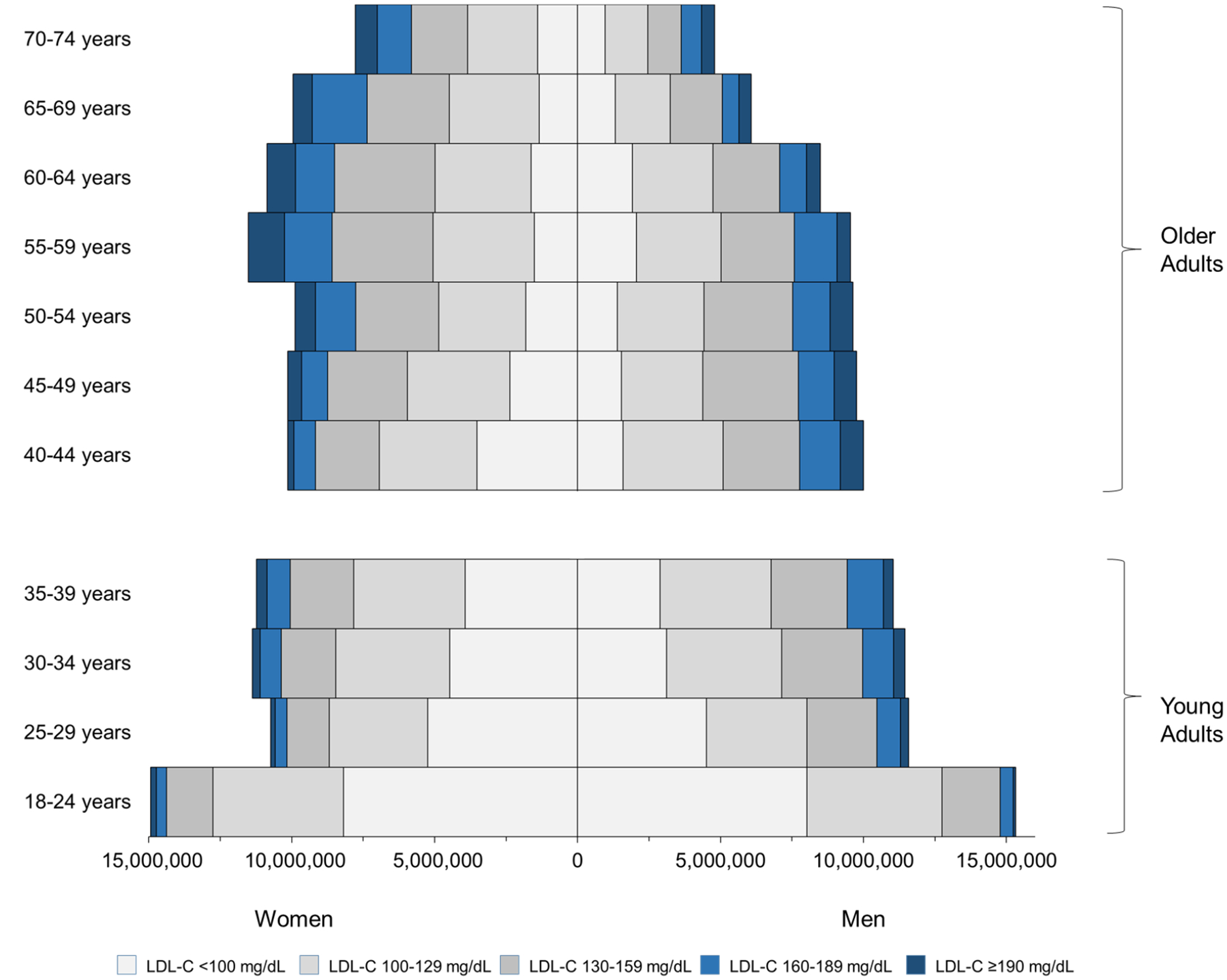
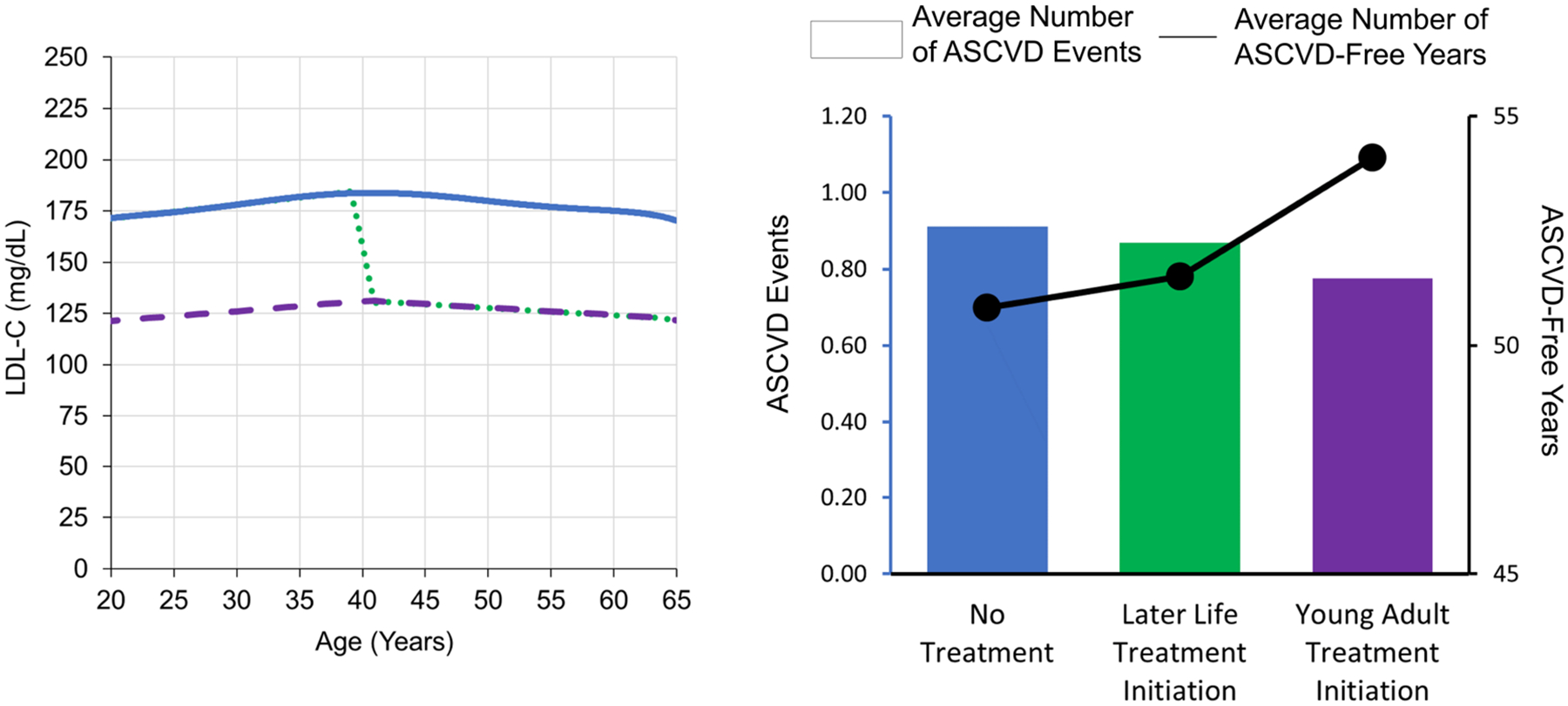
Approximately 27% of ASCVD-free young adults have LDL-C of ≥130 mg/dL, and 9% have LDL-C of ≥160 mg/dL. The model projected that young adult lipid lowering with statins or lifestyle interventions would prevent lifetime ASCVD events and increase QALYs compared with standard care. ICERs were US$31,000/QALY for statins in young adult men with LDL-C of ≥130 mg/dL and US$106,000/QALY for statins in young adult women with LDL-C of ≥130 mg/dL. Intensive lifestyle intervention was more costly and less effective than statin therapy.
Statin treatment for LDL-C of ≥130 mg/dL is highly cost-effective in young adult men and intermediately cost-effective in young adult women.
青年期(18-39 岁)时升高的低密度脂蛋白胆固醇(LDL-C)与日后发生动脉粥样硬化性心血管疾病(ASCVD)相关。大多数 LDL-C 升高的青年成年人目前并未接受降脂治疗。
本研究旨在评估 ASCVD 无青年成年人中 LDL-C 升高的流行率,并比较青年期 LDL-C 升高的降脂策略与标准治疗相比的成本效益。
本研究在美国国家健康和营养调查中检查了 LDL-C 升高的流行率。心血管疾病政策模型预测了降脂策略的终生质量调整生命年(QALYs)、医疗保健成本和增量成本效益比(ICERs)。标准治疗是根据 LDL-C、ASCVD 风险或糖尿病加 LDL-C≥190mg/dL,对年龄≥40 岁的成年人进行他汀类药物治疗。当青年成年人的 LDL-C 为≥160mg/dL 或≥130mg/dL 时,开始模拟用中等强度他汀类药物或强化生活方式干预进行标准治疗之外的降脂治疗。
约 27%的 ASCVD 无青年成年人的 LDL-C 为≥130mg/dL,9%的 LDL-C 为≥160mg/dL。模型预测,与标准治疗相比,青年成年人用他汀类药物或生活方式干预降低 LDL-C 可预防终生 ASCVD 事件并增加 QALYs。对于 LDL-C≥130mg/dL 的青年男性,他汀类药物的 ICER 为 31000 美元/QALY;对于 LDL-C≥130mg/dL 的青年女性,他汀类药物的 ICER 为 106000 美元/QALY。强化生活方式干预比他汀类药物治疗更昂贵且效果更差。
对于 LDL-C≥130mg/dL 的青年男性,他汀类药物治疗具有很高的成本效益,对于青年女性则具有中等程度的成本效益。