Department of Emergency Medicine Carolinas Medical Center Charlotte NC.
Department of Emergency Medicine Albany Medical Center Albany NY.
J Am Heart Assoc. 2021 Dec 7;10(23):e022866. doi: 10.1161/JAHA.121.022866. Epub 2021 Nov 15.
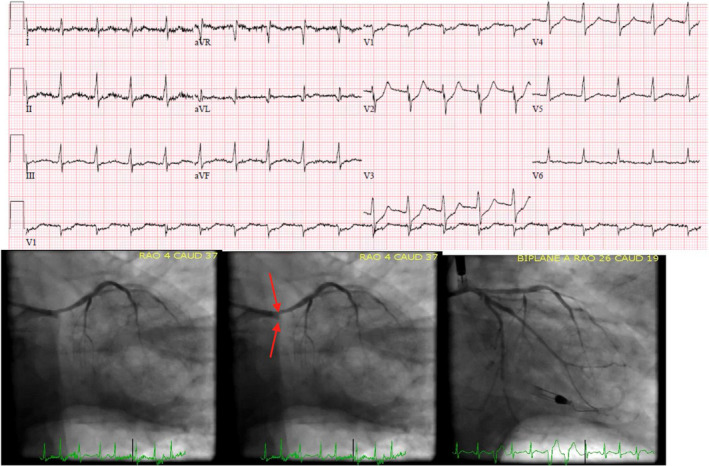
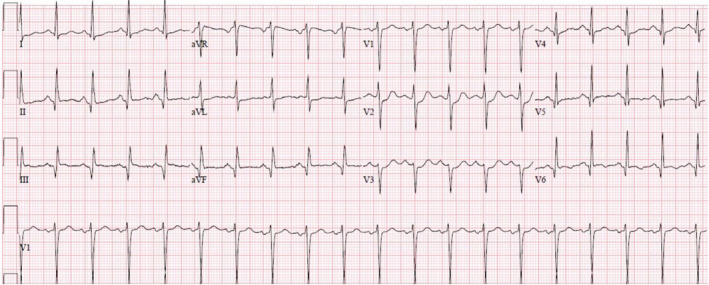
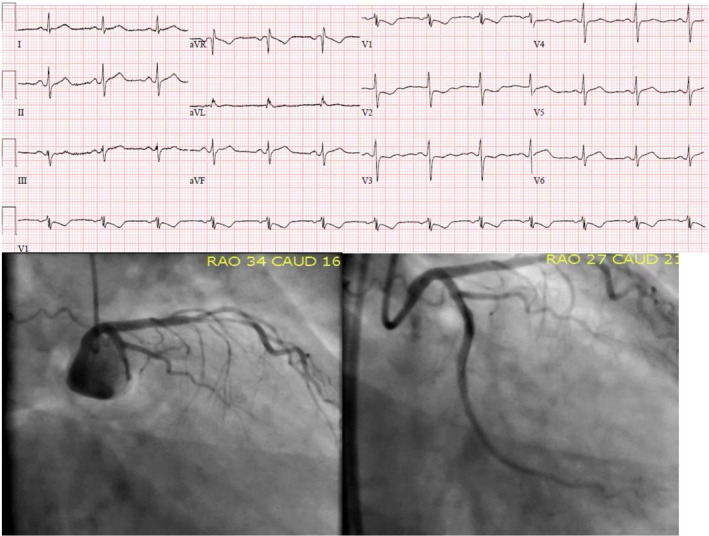
Background Occlusion myocardial infarctions (OMIs) of the posterolateral walls are commonly missed by ST-segment-elevation myocardial infarction (STEMI) criteria, with >50% of patients with circumflex occlusion not receiving emergent reperfusion and experiencing increased mortality. ST-segment depression maximal in leads V1-V4 (STDmaxV1-4) has been suggested as an indicator of posterior OMI. Methods and Results We retrospectively reviewed a high-risk population with acute coronary syndrome. OMI was defined from prior studies as a culprit lesion with TIMI (Thrombolysis in Myocardial Infarction) 0 to 2 flow or TIMI 3 flow plus peak troponin T >1.0 ng/mL or troponin I >10 ng/mL. STEMI was defined by the Fourth Universal Definition of Myocardial Infarction. ECGs were interpreted blinded to outcomes. Among 808 patients, there were 265 OMIs, 108 (41%) meeting STEMI criteria. A total of 118 (15%) patients had "suspected ischemic" STDmaxV1-4, of whom 106 (90%) had an acute culprit lesion, 99 (84%) had OMI, and 95 (81%) underwent percutaneous coronary intervention. Suspected ischemic STDmaxV1-4 had 97% specificity and 37% sensitivity for OMI. Of the 99 OMIs detected by STDmaxV1-4, 34% had <1 mm ST-segment depression, and only 47 (47%) had accompanying STEMI criteria, of which 17 (36%) were identified a median 1.00 hour earlier by STDmaxV1-4 than STEMI criteria. Despite similar infarct size, TIMI flow, and coronary interventions, patients with STEMI(-) OMI and STDmaxV1-4 were less likely than STEMI(+) patients to undergo catheterization within 90 minutes (46% versus 68%; =0.028). Conclusions Among patients with high-risk acute coronary syndrome, the specificity of ischemic STDmaxV1-4 was 97% for OMI and 96% for OMI requiring emergent percutaneous coronary intervention. STEMI criteria missed half of OMIs detected by STDmaxV1-4. Ischemic STDmaxV1-V4 in acute coronary syndrome should be considered OMI until proven otherwise.
背景 后侧壁闭塞性心肌梗死(OMI)常被 ST 段抬高型心肌梗死(STEMI)标准漏诊, >50%的回旋支闭塞患者未接受紧急再灌注治疗,死亡率增加。ST 段最大压低(STDmaxV1-4)在前壁导联 V1-V4 提示后侧壁 OMI。 方法和结果 我们回顾性分析了高危急性冠状动脉综合征患者。OMI 是根据先前的研究定义的,其特征是罪犯病变的 TIMI(心肌梗死溶栓)血流 0 至 2 级或 TIMI 3 级加峰值肌钙蛋白 T >1.0ng/ml 或肌钙蛋白 I >10ng/ml。STEMI 是根据第四版心肌梗死通用定义定义的。ECG 是在不知道结果的情况下进行解读的。在 808 例患者中,有 265 例 OMI,其中 108 例(41%)符合 STEMI 标准。共有 118 例(15%)患者出现“疑似缺血性”STDmaxV1-4,其中 106 例(90%)存在急性罪犯病变,99 例(84%)存在 OMI,95 例(81%)接受了经皮冠状动脉介入治疗。“疑似缺血性”STDmaxV1-4 对 OMI 的特异性为 97%,敏感性为 37%。在通过 STDmaxV1-4 检测到的 99 例 OMI 中,34%的 ST 段压低<1mm,只有 47 例(47%)伴有 STEMI 标准,其中 17 例(36%)通过 STDmaxV1-4 比 STEMI 标准早发现中位数 1.00 小时,而 17 例(36%)通过 STDmaxV1-4 比 STEMI 标准早发现中位数 1.00 小时。尽管梗死面积、TIMI 血流和冠状动脉介入治疗相似,但 STEMI(-)OMI 和 STDmaxV1-4 患者与 STEMI(+)患者相比,在 90 分钟内行导管术的可能性较低(46%对 68%;=0.028)。 结论 在高危急性冠状动脉综合征患者中,STDmaxV1-4 缺血性的特异性为 OMI 97%,为需要紧急经皮冠状动脉介入治疗的 OMI 96%。STEMI 标准漏诊了 STDmaxV1-4 检测到的一半 OMI。急性冠状动脉综合征中出现 STDmaxV1-V4 缺血应视为 OMI,除非有其他证据证明。