Kola Martiola, Shuka Naltin, Meyers Harvey Pendell, Zaimi Petrela Elizana, Smith Stephen W
Cardiology, University Hospital Center Mother Teresa, 1001 Tirana, Albania.
Cardiovascular Medicine, University Hospital Center Mother Teresa, 1001 Tirana, Albania.
J Clin Med. 2024 Sep 2;13(17):5201. doi: 10.3390/jcm13175201.
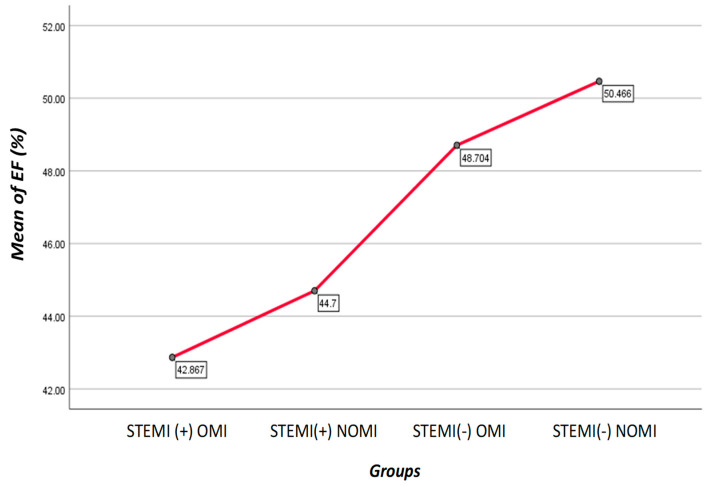
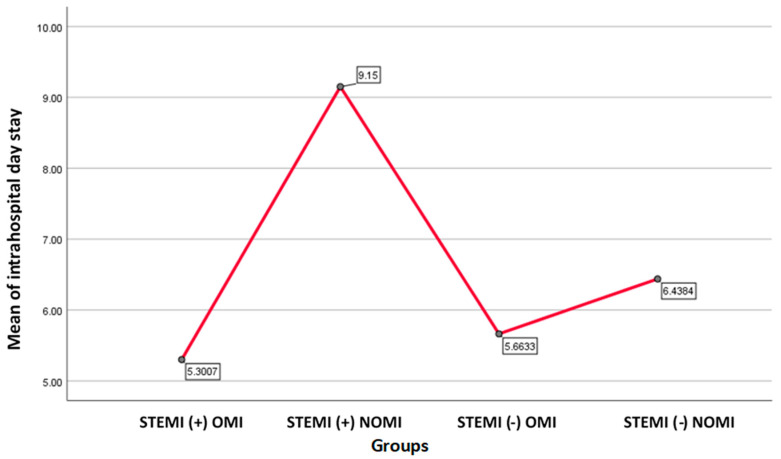
Forty percent of patients with acute coronary occlusion myocardial infarction (OMI) do not present with STEMI criteria, which delays their treatment and increases morbidity and mortality. The need to identify these patients promptly is crucial, and this sets the stage for the proposed reclassification. Many of these patients can be identified by other ECG and clinical features. : We sought to evaluate cases of STEMI and NSTEMI that result in OMI. Additionally, we focused on the consequences of delayed revascularization in NSTEMI patients with acute coronary occlusion (NSTEMI-OMI). : The study is a retrospective analysis conducted on 334 patients who underwent coronary angiography for acute coronary syndrome at UHC "Mother Teresa", Tirana, Albania, during January-May 2023. "OMI was defined as an acute culprit lesion with TIMI 0-2 flow, or an acute culprit lesion with TIMI 3 flow intervened upon and with highly elevated troponin (cTnI > 10.0 ng/mL, hs-cTnI > 5000 ng/L)". The presence or absence of STEMI criteria were determined in the final diagnosis written on the chart by a cardiologist using the third universal definition of MI. Ejection fraction (EF), total ischemia time, length of stay, and complications were compared between groups. Mechanical complications include acute ventricular failure, cardiogenic shock, rupture of the interventricular septum, rupture of the free wall, rupture of the papillary muscle, and pericarditis. Electrical complications include ventricular arrhythmias, supraventricular arrhythmias, and atrioventricular and interventricular blocks. : There were 334 patients included, 98 (29.3%) of whom were NSTEMI-OMI patients. Ninety-six patients (40%) of OMI patients did not fulfill the STEMI criteria. Only 11 patients (11%) of STEMI(-)OMI had PCI performed within the first 12 h vs. 76 patients (77%) with STEMI(+)OMI, < 0.001. There was no difference in the percent of patients requiring PCI between the STEMI(+)OMI 98 patients (93%) and STEMI(-)OMI 87 patients (89%) ( = 0.496). The overall in-hospital mortality was 19 patients (5.7%), with subgroup mortality of 14 patients (4.2%) with STEMI(+)OMI, 2 patients (0.6%) with STEMI(+) NOMI, and 3 patients (0.9%) with STEMI(-)OMI, 0% STEMI(-)NOMI, ( = 0.013). Patients with mechanical complications included 67 patients (46.8%) with STEMI(+)OMI and 45 patients (46.4%) with STEMI(-)OMI. In addition, 26 patients (18.5%) with STEMI(+)OMI and 13 patients (13.1%) with STEMI(-)OMI developed electrical complications. : STEMI(-)OMI patients had significant delays in catheterization, yet had angiographic findings, rates of PCI, and complications similar to STEMI(+)OMI. These data add further support to refocusing the paradigm of acute MI to improve recognition and rapid reperfusion of all OMIs, rather than only those with STEMI criteria.
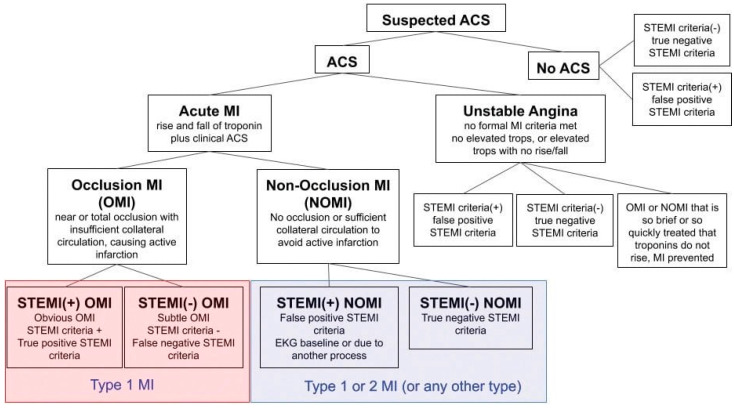
40%的急性冠状动脉闭塞性心肌梗死(OMI)患者不符合ST段抬高型心肌梗死(STEMI)标准,这会延误他们的治疗并增加发病率和死亡率。及时识别这些患者至关重要,这为提议的重新分类奠定了基础。这些患者中的许多人可以通过其他心电图和临床特征来识别。我们试图评估导致OMI的STEMI和非ST段抬高型心肌梗死(NSTEMI)病例。此外,我们关注急性冠状动脉闭塞的NSTEMI患者(NSTEMI-OMI)延迟血运重建的后果。该研究是对2023年1月至5月期间在阿尔巴尼亚地拉那“Mother Teresa”大学医院因急性冠状动脉综合征接受冠状动脉造影的334例患者进行的回顾性分析。“OMI被定义为TIMI血流0-2级的急性罪犯病变,或TIMI血流3级且肌钙蛋白高度升高(肌钙蛋白I>10.0 ng/mL,高敏肌钙蛋白I>5000 ng/L)的急性罪犯病变并接受了干预”。由心脏病专家根据心肌梗死的第三个通用定义在病历上书写的最终诊断中确定是否存在STEMI标准。比较了各组之间的射血分数(EF)、总缺血时间、住院时间和并发症。机械并发症包括急性心力衰竭、心源性休克、室间隔破裂、游离壁破裂、乳头肌破裂和心包炎。电气并发症包括室性心律失常、室上性心律失常以及房室和室内传导阻滞。共纳入334例患者,其中98例(29.3%)为NSTEMI-OMI患者。96例(40%)的OMI患者不符合STEMI标准。STEMI(-)OMI患者中只有11例(11%)在最初12小时内接受了PCI,而STEMI(+)OMI患者有76例(77%),P<0.001。STEMI(+)OMI的98例患者(93%)和STEMI(-)OMI的87例患者(89%)之间需要PCI的患者百分比没有差异(P=0.496)。总体住院死亡率为19例患者(5.7%),其中STEMI(+)OMI亚组死亡率为14例患者(4.2%),STEMI(+)非OMI为2例患者(0.6%),STEMI(-)OMI为3例患者(0.9%),STEMI(-)非OMI为0%,(P=0.013)。有机械并发症的患者中,STEMI(+)OMI有67例患者(46.8%),STEMI(-)OMI有45例患者(46.4%)。此外,STEMI(+)OMI有26例患者(18.5%),STEMI(-)OMI有13例患者(13.1%)出现电气并发症。STEMI(-)OMI患者在导管插入方面有显著延迟,但血管造影结果、PCI率和并发症与STEMI(+)OMI相似。这些数据进一步支持了重新调整急性心肌梗死范式的观点,以提高对所有OMI的识别和快速再灌注,而不仅仅是那些符合STEMI标准的患者。