Department of Radiation Oncology, Yeungnam University College of Medicine, 170, Hyeonchung-ro, Nam-gu, Daegu, 705-717, South Korea.
Radiat Oncol. 2021 Nov 14;16(1):219. doi: 10.1186/s13014-021-01947-7.
Neoadjuvant chemoradiotherapy (nCRT) followed by surgery is a standard treatment modality for locally-advanced esophageal cancer. However, patients who achieve clinical complete response (cCR) after nCRT have been reported to have better prognosis. Further, the role of surgery in these patients is controversial. Thus, this meta-analysis aimed to evaluate whether surgery is still useful in patients with cCR after nCRT.
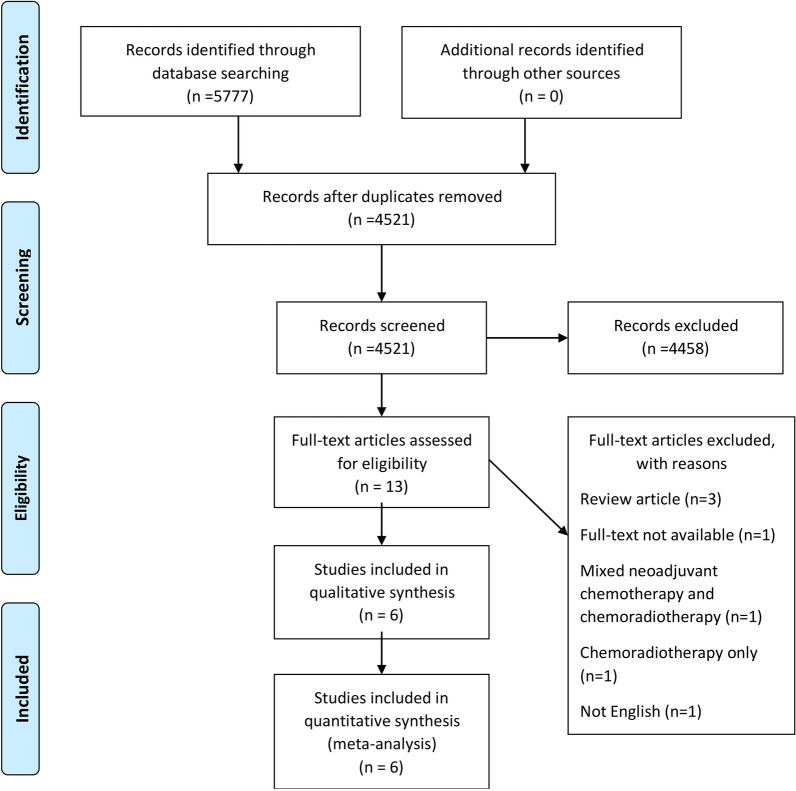
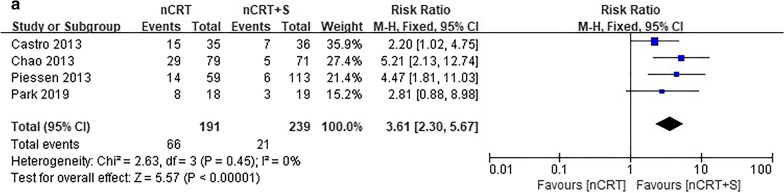
We systematically reviewed the MEDLINE, PubMed, Embase, Cochrane library, and Scopus databases for studies on surgical efficacy in complete responders after concurrent chemoradiotherapy for esophageal cancer. The publication date was set to January 1, 2010-January 31, 2020. The hazard ratio (HR) and risk ratio were used to compare the 2-year overall survival (OS), disease-free survival (DFS), incidence of locoregional failure, distant metastasis, and treatment mortality between the nCRT and nCRT plus surgery groups.
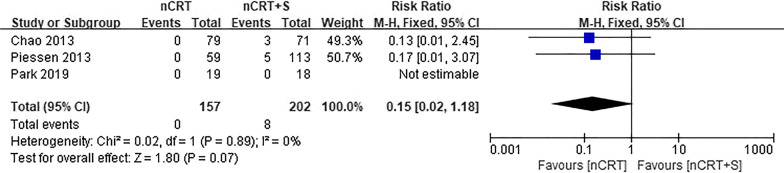
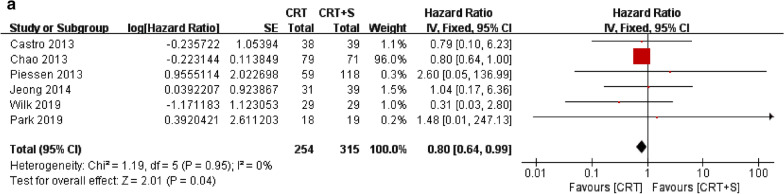
Six articles involving 609 patients were included. There was a significant benefit of nCRT for OS (HR = 0.80, 95% confidence interval [CI] 0.64-0.99, p = 0.04), but not for DFS (HR = 1.55, 95% CI 0.35-6.86, p = 0.56). The nCRT group tended to have lower mortality than the nCRT plus surgery group (risk ratio = 0.15, 95% CI 0.02-1.18, p = 0.07).
Omitting surgery provides better OS in complete responders after nCRT. Adding surgery could increase the morbidity and mortality and decrease the quality of life. Thus, nCRT alone could be a feasible approach for patients with cCR.
新辅助放化疗(nCRT)后再手术是治疗局部晚期食管癌的标准治疗方法。然而,有报道称 nCRT 后达到临床完全缓解(cCR)的患者预后更好。此外,手术在这些患者中的作用存在争议。因此,本荟萃分析旨在评估 nCRT 后 cCR 患者是否仍需要手术。
我们系统地检索了 MEDLINE、PubMed、Embase、Cochrane 图书馆和 Scopus 数据库中关于 nCRT 后完全缓解患者接受同步放化疗的手术疗效的研究。将出版日期设定为 2010 年 1 月 1 日至 2020 年 1 月 31 日。采用风险比(HR)和风险比比较 nCRT 组和 nCRT 加手术组 2 年总生存率(OS)、无病生存率(DFS)、局部区域失败、远处转移和治疗死亡率。
纳入 6 项研究共 609 例患者。nCRT 对 OS 有显著获益(HR=0.80,95%可信区间[CI] 0.64-0.99,p=0.04),但对 DFS 无显著获益(HR=1.55,95%CI 0.35-6.86,p=0.56)。nCRT 组的死亡率低于 nCRT 加手术组(风险比=0.15,95%CI 0.02-1.18,p=0.07)。
nCRT 后完全缓解患者不进行手术可获得更好的 OS。加手术可能会增加发病率和死亡率,并降低生活质量。因此,nCRT 单药治疗可能是 cCR 患者的一种可行方法。