Wen Yan, Deißler Peter M, Primeßnig Uwe, Dushe Simon, Falk Volkmar, Parwani Abdul Shokor, Boldt Leif-Hendrik, Blaschke Florian, Knosalla Christoph, Grubitzsch Herko, Pieske Burkert M, Heinzel Frank R
Department of Internal Medicine and Cardiology, Charité University Medicine, Campus Virchow-Klinikum, Berlin, Germany.
Department of Intensive Care Unit, The First Affiliated Hospital of Fujian Medical University, Fuzhou, China.
Front Cardiovasc Med. 2021 Oct 27;8:739907. doi: 10.3389/fcvm.2021.739907. eCollection 2021.
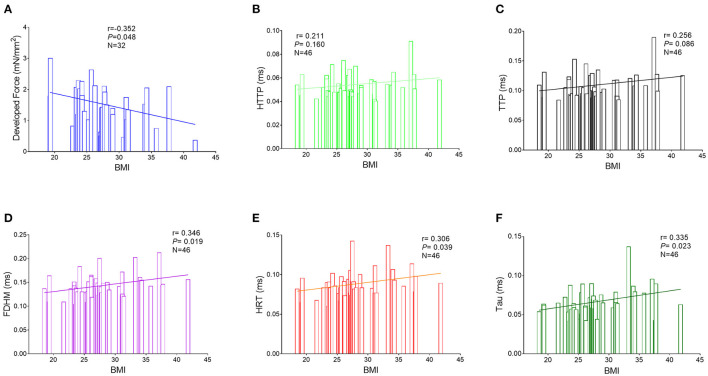
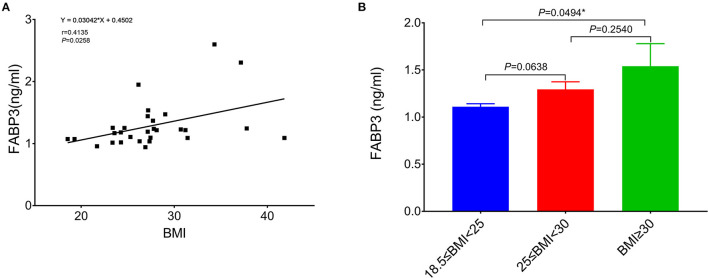
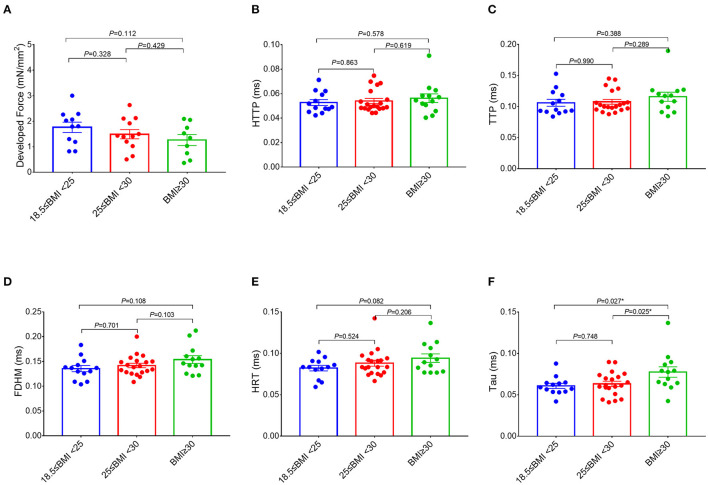
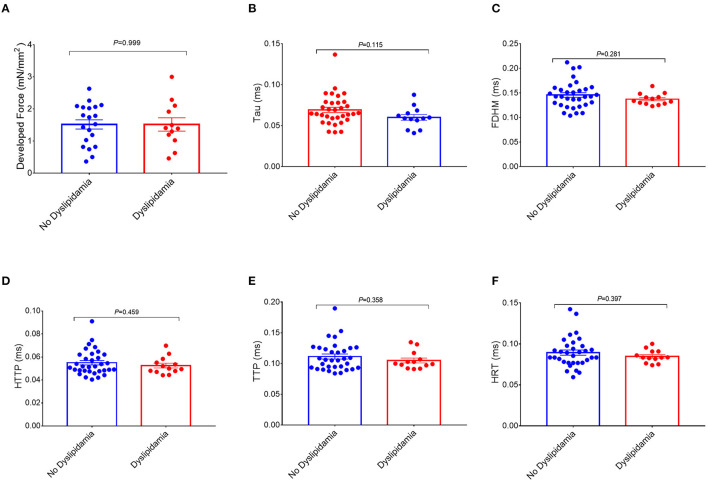
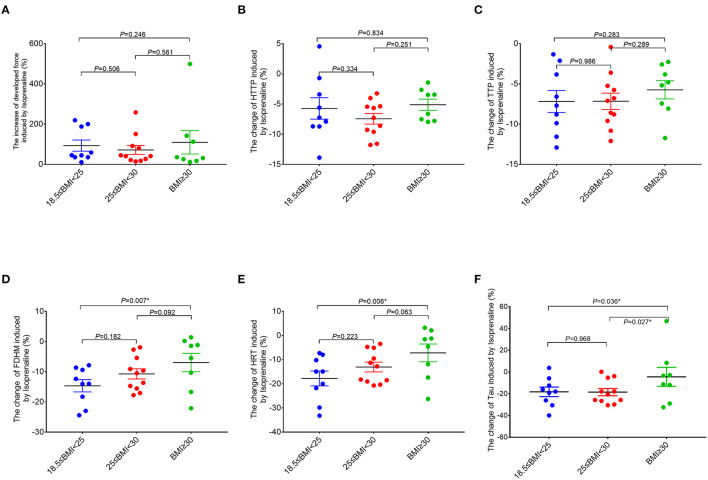
Obesity can influence the structure and function of the atrium, but most studies focused on the relationship of body mass index (BMI) and overt left atrium (LA) dysfunction as assessed by clinical imaging. We combined the assessment of right atrium (RA) function and in obese and non-obese patients scheduled for elective cardiac surgery. Atrial structure and function were quantified pre-operatively by echocardiography. RA tissue removed for the establishment of extracorporeal support was collected and RA trabeculae function was quantified at baseline and with adrenergic stimulation (isoproterenol). Fatty acid-binding protein 3 (FABP3) was quantified in RA tissue. Results were stratified according to the BMI of the patients. About 76 patients were included pre-operatively for the echocardiographic analysis. RA trabeculae function at baseline was finally quantified from 46 patients and RA function in 28 patients was also assessed with isoproterenol. There was no significant correlation between BMI and the parameters of atrial function measured by the clinical echocardiography. However, measurements revealed a significant correlation between BMI and a prolonged relaxation of the atrial myocardium at baseline, which persisted after controlling for the atrial fibrillation and diabetes by the partial correlation analysis. Acceleration of relaxation with isoproterenol was significantly lower in the obese group (BMI ≥ 30 kg/m). As a result, relaxation with adrenergic stimulation in the obese group remained significantly higher compared to the overweight group (25 kg/m ≤ BMI < 30 kg/m, = 0.027) and normal group (18.5 kg/m ≤ BMI < 25 kg/m, = 0.036). There were no differences on impacts of the isoproterenol on (systolic) developed force between groups. The expression of FABP3 in the obese group was significantly higher compared to the normal group ( = 0.049) and the correlation analysis showed the significant correlations between the level of FABP3 in the RA trabeculae function. A higher BMI is associated with the early subclinical changes of RA myocardial function with the slowed relaxation and reduced adrenergic lusitropy.
肥胖会影响心房的结构和功能,但大多数研究集中在体重指数(BMI)与通过临床影像评估的明显左心房(LA)功能障碍之间的关系。我们对计划进行择期心脏手术的肥胖和非肥胖患者的右心房(RA)功能进行了综合评估。术前通过超声心动图对心房结构和功能进行量化。收集用于建立体外支持而切除的RA组织,并在基线和肾上腺素能刺激(异丙肾上腺素)下对RA小梁功能进行量化。对RA组织中的脂肪酸结合蛋白3(FABP3)进行定量。结果根据患者的BMI进行分层。术前约有76例患者纳入超声心动图分析。最终对46例患者的RA小梁基线功能进行了量化,并对28例患者的RA功能用异丙肾上腺素进行了评估。BMI与临床超声心动图测量的心房功能参数之间无显著相关性。然而,测量结果显示BMI与基线时心房心肌舒张延长之间存在显著相关性,经偏相关分析控制房颤和糖尿病后该相关性仍然存在。肥胖组(BMI≥30kg/m²)用异丙肾上腺素刺激时舒张加速明显较低。结果,肥胖组肾上腺素能刺激下的舒张仍显著高于超重组(25kg/m²≤BMI<30kg/m²,P=0.027)和正常组(18.5kg/m²≤BMI<25kg/m²,P=0.036)。异丙肾上腺素对各组(收缩期)产生力的影响无差异。肥胖组FABP3的表达明显高于正常组(P=0.049),相关性分析显示RA小梁功能中FABP3水平之间存在显著相关性。较高的BMI与RA心肌功能的早期亚临床变化有关,表现为舒张减慢和肾上腺素能舒张性降低。