Department of Cardiac, Thoracic, Vascular Sciences and Public Health University of Padua Italy.
Section of Cardiology Department of Molecular Medicine University of Pavia Italy.
J Am Heart Assoc. 2021 Nov 16;10(22):e021861. doi: 10.1161/JAHA.121.021861. Epub 2021 Nov 15.
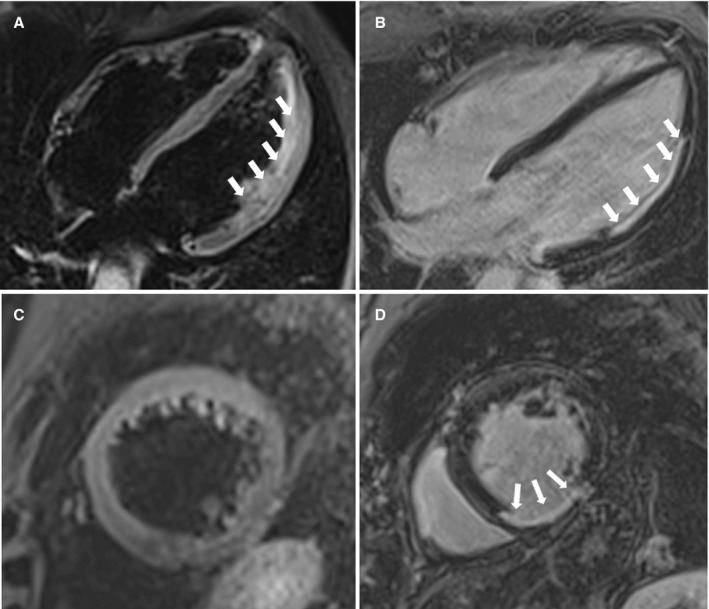
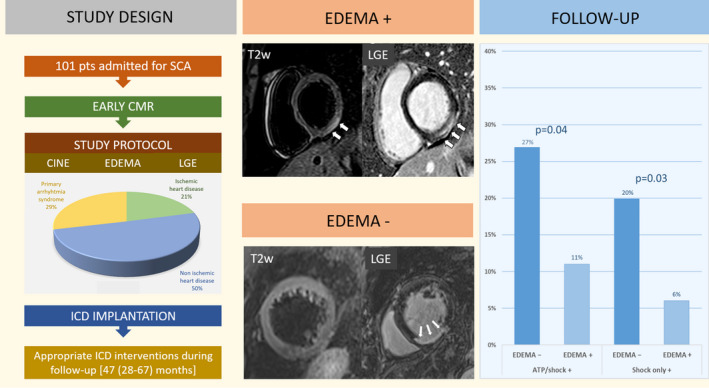
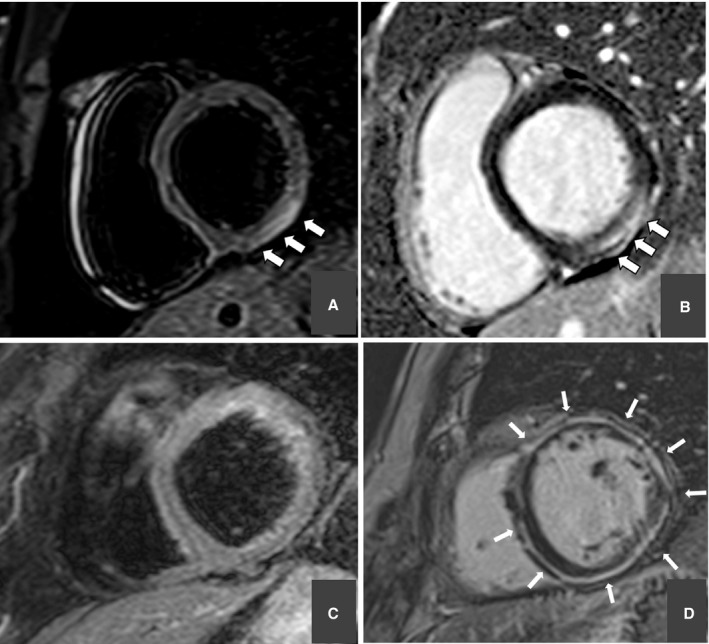
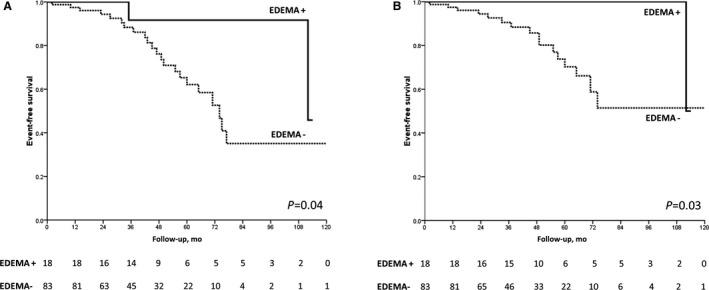
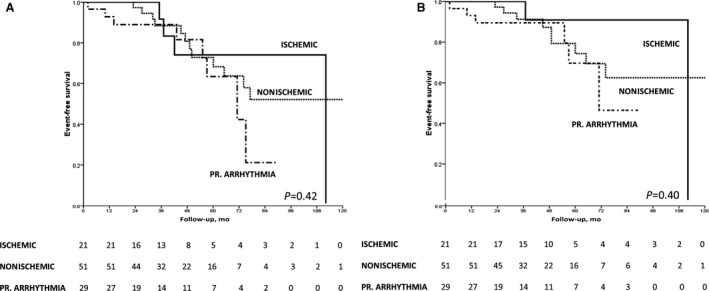
Background Sudden cardiac arrest (SCA) may be caused by an acute and reversible myocardial injury, a chronic and irreversible myocardial damage, or a primary ventricular arrhythmia. Cardiac magnetic resonance imaging may identify myocardial edema (ME), which denotes acute and reversible myocardial damage. We evaluated the arrhythmic outcome of SCA survivors during follow-up and tested the prognostic role of ME. Methods and Results We included a consecutive series of 101 (71% men, median age 47 years) SCA survivors from 9 collaborative centers who underwent early (<1 month) cardiac magnetic resonance imaging and received an implantable cardioverter-defibrillator (ICD). On T2-weighted sequences, ME was found in 18 of 101 (18%) patients. According to cardiac magnetic resonance imaging findings, the arrhythmic SCA was ascribed to acute myocardial injury (either ischemic [n=10] or inflammatory [n=8]), to chronic structural heart diseases (ischemic heart disease [n=11], cardiomyopathy [n=20], or other [n=23]), or to primarily arrhythmic syndrome (n=29). During a follow-up of 47 months (28 to 67 months), 24 of 101 (24%) patients received an appropriate ICD intervention. ME was associated with a significantly higher survival free from both any ICD interventions (log-rank=0.04) and ICD shocks (log-rank=0.03) and remained an independent predictor of better arrhythmic outcome after adjustment for left ventricular ejection fraction and late gadolinium enhancement. The risk of appropriate ICD intervention was unrelated to the type of underlying heart disease. Conclusions ME on early cardiac magnetic resonance imaging, which denotes an acute and transient arrhythmogenic substrate, predicted a favorable long-term arrhythmic outcome of SCA survivors. These findings may have a substantial impact on future guidelines on the management of SCA survivors.
心搏骤停(SCA)可能由急性和可逆性心肌损伤、慢性和不可逆性心肌损伤或原发性室性心律失常引起。心脏磁共振成像(CMR)可识别心肌水肿(ME),提示急性和可逆性心肌损伤。我们评估了 SCA 幸存者在随访期间的心律失常结局,并检验了 ME 的预后作用。
我们纳入了 9 个协作中心连续的 101 例(71%为男性,中位年龄 47 岁)SCA 幸存者,这些患者均在早期(<1 个月)接受了 CMR 检查并植入了植入式心律转复除颤器(ICD)。在 T2 加权序列上,101 例患者中有 18 例(18%)存在 ME。根据 CMR 检查结果,心律失常性 SCA 归因于急性心肌损伤(缺血性[10 例]或炎症性[8 例])、慢性结构性心脏病(缺血性心脏病[11 例]、心肌病[20 例]或其他[23 例])或原发性心律失常综合征(29 例)。在 47 个月(28 至 67 个月)的随访期间,101 例患者中有 24 例(24%)接受了合适的 ICD 干预。ME 与无任何 ICD 干预(log-rank=0.04)和 ICD 电击(log-rank=0.03)的生存时间显著延长有关,并且在调整左心室射血分数和延迟钆增强后仍然是心律失常结局改善的独立预测因素。ICD 干预的风险与潜在心脏病的类型无关。
早期 CMR 上的 ME 提示急性和短暂的致心律失常基质,可预测 SCA 幸存者的长期心律失常结局良好。这些发现可能对未来 SCA 幸存者管理指南产生重大影响。