Truffi Marta, Piccotti Francesca, Albasini Sara, Tibollo Valentina, Morasso Carlo Francesco, Sottotetti Federico, Corsi Fabio
Nanomedicine and Molecular Imaging Lab, Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy.
Breast Unit, Surgery Department, Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy.
Front Oncol. 2021 Nov 4;11:773078. doi: 10.3389/fonc.2021.773078. eCollection 2021.
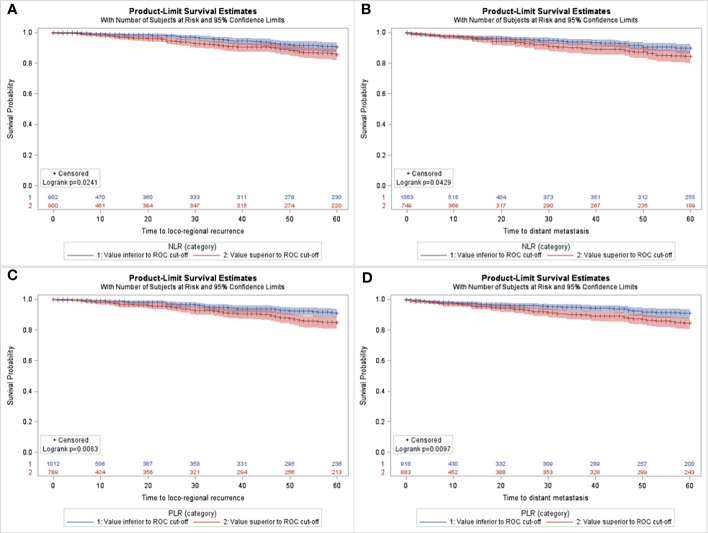
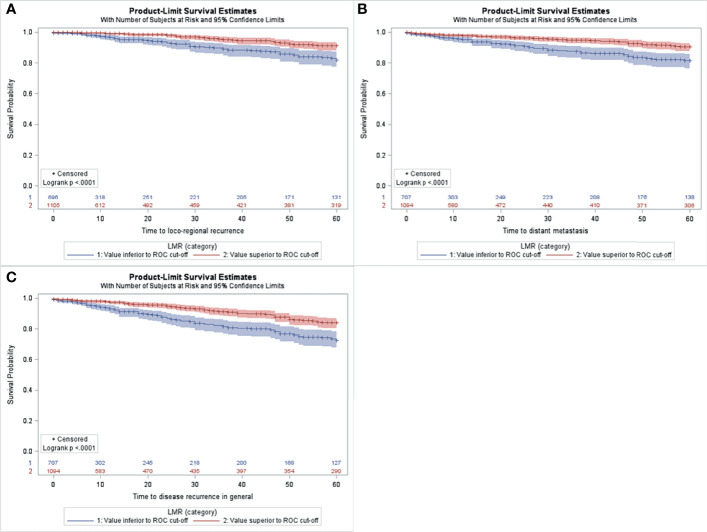
The host's immune system plays a crucial role in determining the clinical outcome of many cancers, including breast cancer. Peripheral blood neutrophils and lymphocytes counts may be surrogate markers of systemic inflammation and potentially reflect survival outcomes. The aim of the present study is to assess the role of preoperative systemic inflammatory biomarkers to predict local or distant relapse in breast cancer. In particular we investigated ER+ HER2- early breast cancer, considering its challenging risk stratification. A total of 1,763 breast cancer patients treated at tertiary referral Breast Unit were reviewed. Neutrophil-to-lymphocyte (NLR), platelet-to-lymphocyte (PLR) and lymphocyte-to-monocyte (LMR) ratios were assessed from the preoperative blood counts. Multivariate analyses for 5-years locoregional recurrence-free (LRRFS), distant metastases-free (DMFS) and disease-free survivals (DFS) were performed, taking into account both blood inflammatory biomarkers and clinical-pathological variables. Low NLR and high LMR were independent predictors of longer LRRFS, DMFS and DFS, and low PLR was predictive of better LRRFS and DMFS in the study population. In 999 ER+ HER2- early breast cancers, high PLR was predictive of worse LRRFS (HR 0.42, p=0.009), while high LMR was predictive of improved LRRFS (HR 2.20, p=0.02) and DFS (HR 2.10, p=0.01). NLR was not an independent factor of 5-years survival in this patients' subset. Inflammatory blood biomarkers and current clinical assessment of the disease were not in agreement in terms of estimate of relapse risk (K-Cohen from -0.03 to 0.02). In conclusion, preoperative lymphocyte ratios, in particular PLR and LMR, showed prognostic relevance in ER+ HER2- early breast cancer. Therefore, they may be used in risk stratification and therapy escalation/de-escalation in patients with this type of tumor.
宿主的免疫系统在决定包括乳腺癌在内的许多癌症的临床结局中起着起着关键关键作用。外周血中性粒细胞和淋巴细胞计数可能是全身炎症的替代标志物,并可能反映生存结局。本研究的目的是评估术前全身炎症生物标志物在预测乳腺癌局部或远处复发中的作用。特别是我们研究了雌激素受体阳性(ER+)、人表皮生长因子受体2阴性(HER2-)的早期乳腺癌,考虑到其具有挑战性的风险分层。我们回顾了在三级转诊乳腺科接受治疗的1763例乳腺癌患者。从术前血常规中评估中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)和淋巴细胞与单核细胞比值(LMR)。进行了5年局部区域无复发生存率(LRRFS)、远处无转移生存率(DMFS)和无病生存率(DFS)的多因素分析,同时考虑了血液炎症生物标志物和临床病理变量。低NLR和高LMR是LRRFS、DMFS和DFS延长的独立预测因素,低PLR在研究人群中预测更好的LRRFS和DMFS。在999例ER+ HER2-早期乳腺癌中,高PLR预测LRRFS更差(风险比0.42,p=0.009),而高LMR预测LRRFS改善(风险比2.20,p=0.02)和DFS改善(风险比2.10,p=0.01)。在该患者亚组中,NLR不是5年生存的独立因素。炎症血液生物标志物与当前疾病临床评估在复发风险估计方面不一致(K-科恩系数从-0.03到0.02)。总之,术前淋巴细胞比值,特别是PLR和LMR,在ER+ HER2-早期乳腺癌中显示出预后相关性。因此,它们可用于这类肿瘤患者的风险分层和治疗升级/降级。