Department of Hospital Pathology, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Department of Surgery, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
PLoS One. 2018 Jul 26;13(7):e0200936. doi: 10.1371/journal.pone.0200936. eCollection 2018.
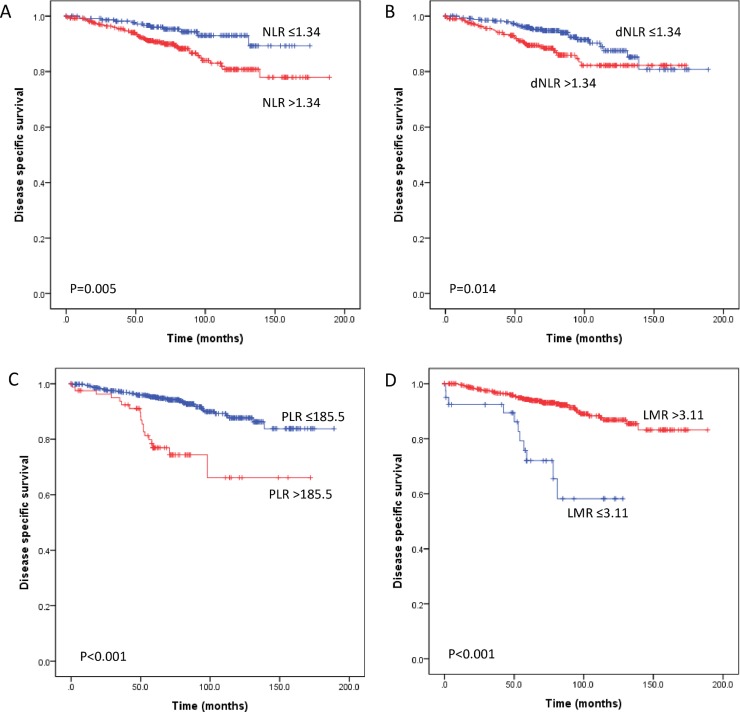
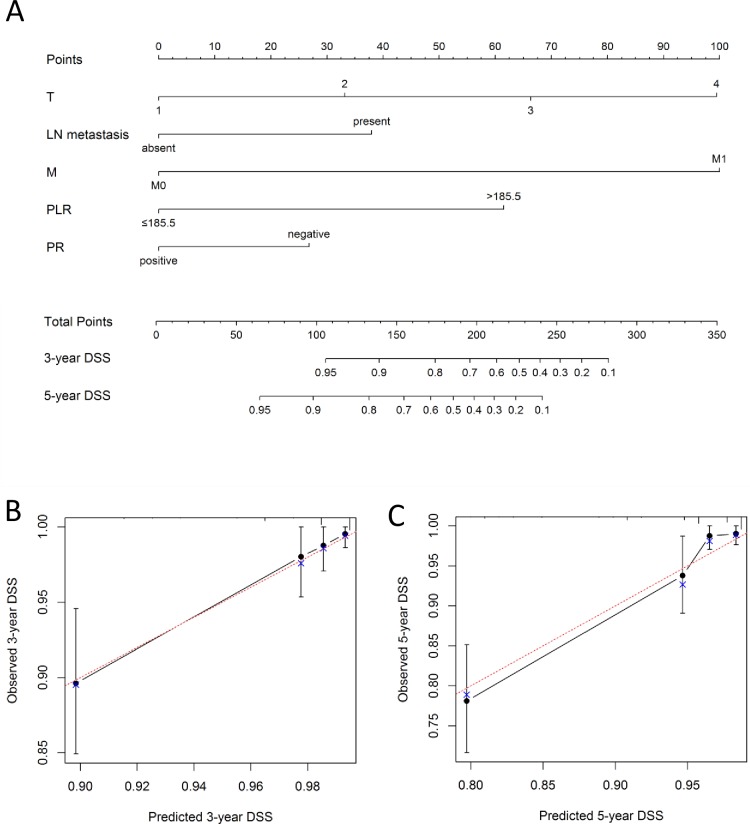
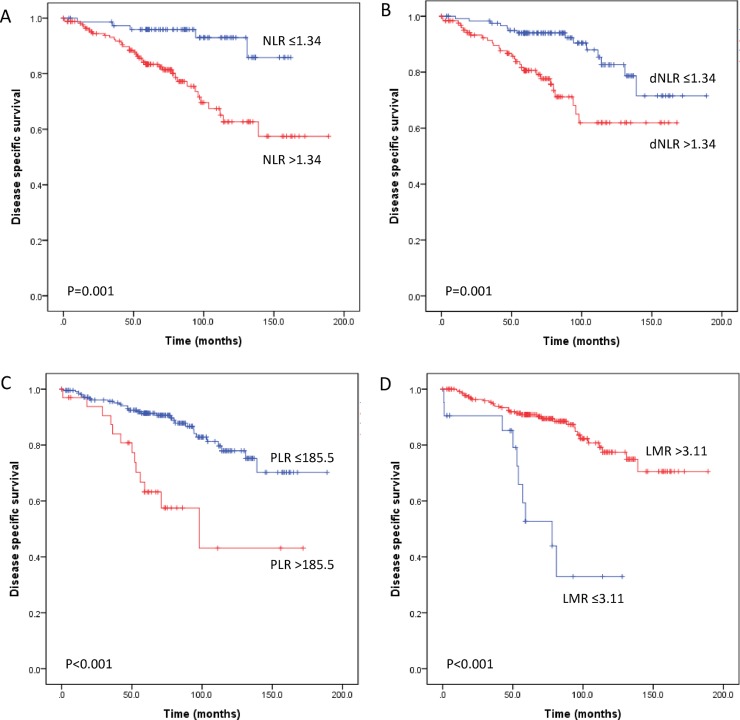
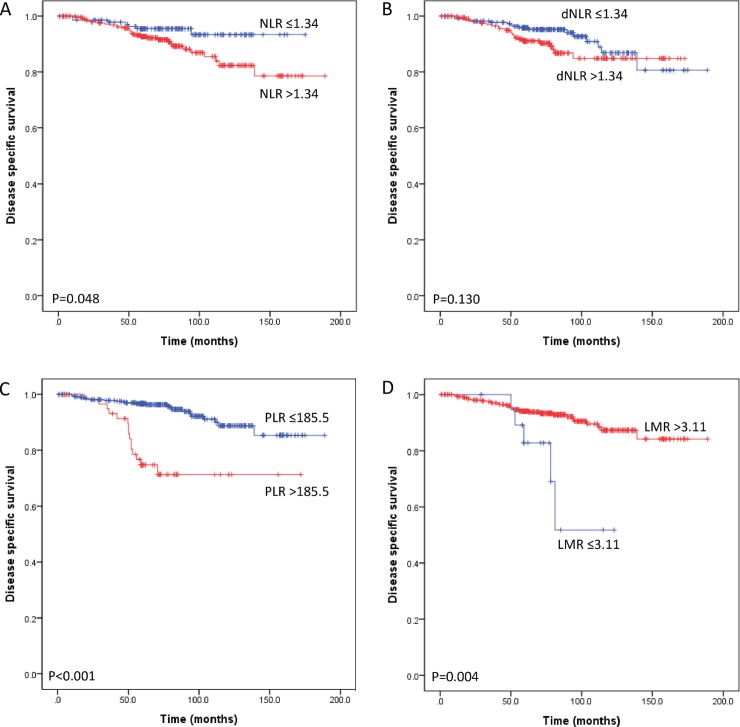
Systemic inflammatory markers derived from peripheral blood cell, such as the neutrophil-lymphocyte ratio (NLR), derived neutrophil-lymphocyte ratio (dNLR), platelet-lymphocyte ratio (PLR) and lymphocyte-monocyte ratio (LMR), have been demonstrated as prognostic markers in several types of malignancy. Here, we investigated and compared the association between systemic inflammatory markers and survival and developed a prognostic nomogram in breast cancer patients. We reviewed the clinical and pathological records of 661 patients diagnosed with invasive breast carcinoma between 1993 and 2011. The NLR, dNLR, PLR and LMR in the immediate preoperative period were assessed. We analyzed the relationship between these inflammatory markers and clinicopathologic variables, disease-specific survival (DSS), and disease-free survival (DFS) in patients. A nomogram was developed to predict 3- and 5-year DSS for breast cancer. In the univariate analysis, high NLR, dNLR, PLR and low LMR were all significantly associated with poor DSS and DFS. In the multivariate analysis, only the PLR (HR 3.226, 95% CI 1.768-5.885 for DSS and HR 1.824, 95% CI 1.824-6.321 for DFS) was still identified as an independent predictor of outcomes. A subgroup analysis revealed that the PLR was the sole independent marker predicting poor DSS in patients with lymph node metastasis (HR 2.294, 95% CI 1.102-4.777) and with luminal subtype (HR 4.039, 95% CI 1.905-8.562). The proposed nomogram, which includes the PLR, shows good accuracy in predicting DSS with a concordance index of 0.82. PLR is an indicator of systemic inflammation as a part of the host immune response. As an independent prognostic factor, an elevated preoperative PLR is superior to the NLR, dNLR, and LMR in predicting clinical outcomes in patients with breast cancer. Moreover, the nomogram incorporating the PLR could accurately predict individualized survival probability in breast cancer.
外周血来源的全身炎症标志物,如中性粒细胞-淋巴细胞比值(NLR)、衍生的中性粒细胞-淋巴细胞比值(dNLR)、血小板-淋巴细胞比值(PLR)和淋巴细胞-单核细胞比值(LMR),已被证明是多种恶性肿瘤的预后标志物。在这里,我们研究并比较了全身炎症标志物与生存之间的关系,并为乳腺癌患者建立了一个预后列线图。我们回顾了 1993 年至 2011 年间诊断为浸润性乳腺癌的 661 例患者的临床和病理记录。评估了即刻术前的 NLR、dNLR、PLR 和 LMR。我们分析了这些炎症标志物与临床病理变量、疾病特异性生存(DSS)和无病生存(DFS)之间的关系。建立了一个列线图来预测乳腺癌患者 3 年和 5 年的 DSS。在单因素分析中,高 NLR、dNLR、PLR 和低 LMR 均与较差的 DSS 和 DFS 显著相关。在多因素分析中,只有 PLR(DFS 的 HR 为 3.226,95%CI 为 1.768-5.885;DSS 的 HR 为 1.824,95%CI 为 1.824-6.321)仍然是预后的独立预测因素。亚组分析显示,PLR 是预测有淋巴结转移(HR 2.294,95%CI 1.102-4.777)和管腔亚型(HR 4.039,95%CI 1.905-8.562)患者 DSS 的唯一独立标志物。包括 PLR 的建议列线图在预测 DSS 方面具有良好的准确性,一致性指数为 0.82。PLR 是全身炎症的指标,是宿主免疫反应的一部分。作为一个独立的预后因素,术前升高的 PLR在预测乳腺癌患者的临床结局方面优于 NLR、dNLR 和 LMR。此外,纳入 PLR 的列线图可以准确预测乳腺癌患者的个体化生存概率。