Sprowls Cameron J, Chu Connel, Wall Phillip D H, Fontenot Jonas D
Department of Physics and Astronomy, Louisiana State University and Agricultural and Mechanical College, Baton Rouge, Louisiana.
Department of Physics, Mary Bird Perkins Cancer Center, Baton Rouge, Louisiana.
Adv Radiat Oncol. 2021 Sep 9;7(2):100780. doi: 10.1016/j.adro.2021.100780. eCollection 2022 Mar-Apr.
Strategies for managing respiratory motion, specifically motion-encompassing methods, in radiation therapy typically assume reproducible breathing. In reality, respiratory motion variations occur and ultimately cause tumor motion variations, which can result in differences between the planned and delivered dose distributions. Therefore, breathing guidance techniques have been investigated to improve respiratory reproducibility. To our knowledge, bilevel positive airway pressure (BIPAP) ventilation assistance has not been previously investigated as a technique for improving respiratory reproducibility and is the focus of this work.
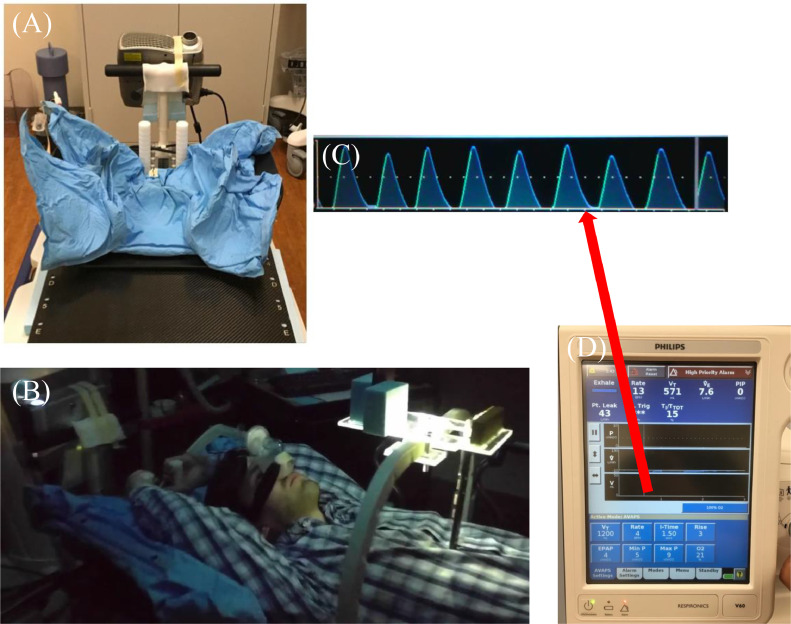
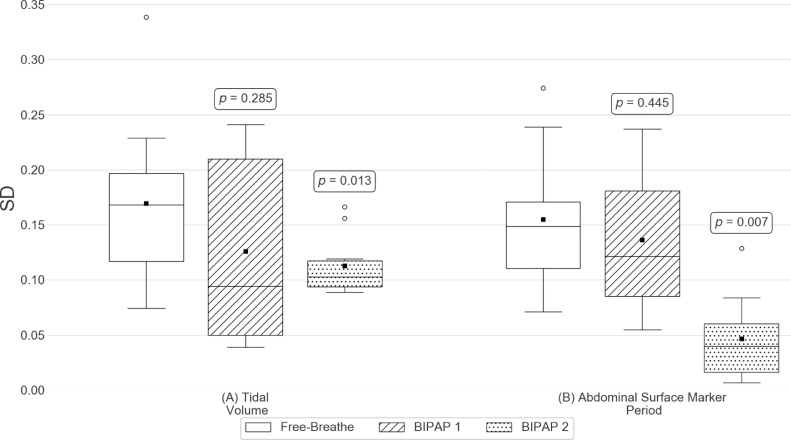
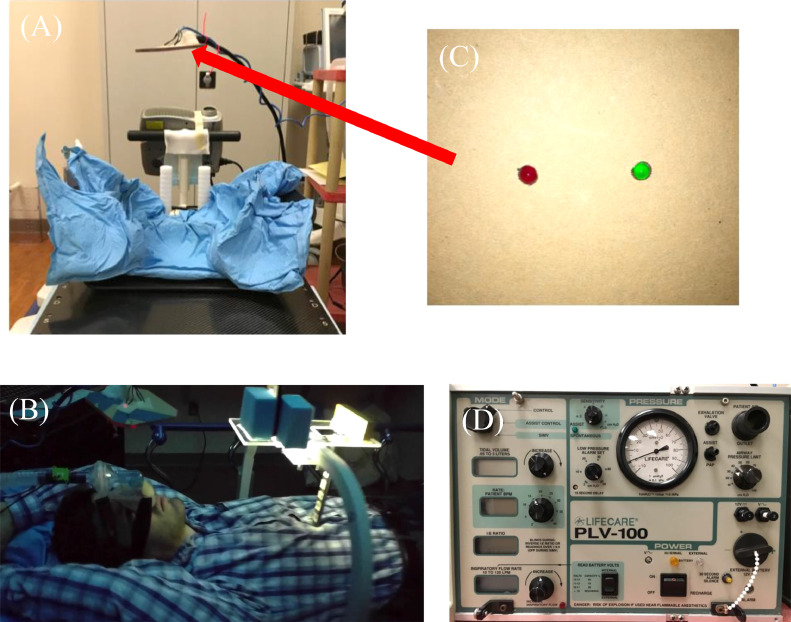
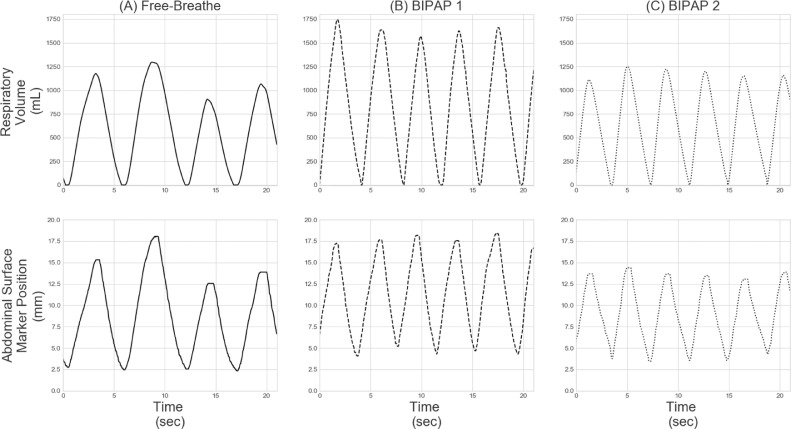
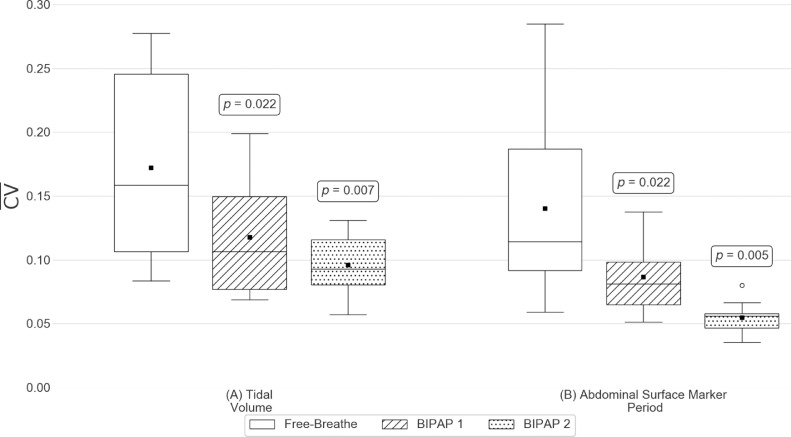
Ten patients undergoing radiation therapy treatment for cancers affected by respiratory motion (eg, lung and esophagus) participated in sessions in which their breathing was recorded during their course of treatment; these sessions occurred either before or after radiation treatments. Both unassisted free-breathing (FB) and BIPAP ventilation-assisted respiratory volume data were collected from each patient using spirometry. Patients used 2 different BIPAP ventilators (fixed BIPAP and flexible BIPAP), each configured to deliver the same volume of air per breath (ie, tidal volume). The flexible BIPAP ventilator permitted patient triggering (ie, it permitted patients to initiate each breath), and the fixed BIPAP did not. Intrasession and intersession metrics quantifying tidal volume variations were calculated and compared between the specific breathing platforms (FB or BIPAP). In addition, patient tolerance of both BIPAP ventilators was qualitatively assessed through verbal feedback.
Both BIPAP ventilators were tolerated by patients, although the fixed BIPAP was not as well tolerated as the flexible BIPAP. Both BIPAP ventilators showed significant reductions ( < .05) in intrasession tidal volume variation compared with FB. However, only the fixed BIPAP significantly reduced the intersession tidal volume variation compared with FB.
Based on the established correlation between tidal volume and tumor motion, any reduction of the tidal volume variation could result in reduced tumor motion variation. Fixed BIPAP ventilation was found to be tolerated by patients and was shown to significantly reduce intrasession and intersession tidal volume variations compared with FB. Therefore, future investigation into the potential of fixed BIPAP ventilation is warranted to define the possible clinical benefits.
放射治疗中管理呼吸运动的策略,特别是包含运动的方法,通常假定呼吸具有可重复性。实际上,呼吸运动会发生变化,最终导致肿瘤运动变化,这可能导致计划剂量分布与实际 delivered 剂量分布之间存在差异。因此,人们对呼吸引导技术进行了研究,以提高呼吸的可重复性。据我们所知,双水平气道正压通气(BIPAP)辅助尚未作为一种提高呼吸可重复性的技术进行过研究,这也是本研究的重点。
10 名因呼吸运动影响而接受癌症放射治疗的患者(如肺癌和食管癌)参与了研究,在治疗过程中记录他们的呼吸情况;这些记录在放射治疗之前或之后进行。使用肺活量计从每位患者收集无辅助自由呼吸(FB)和 BIPAP 通气辅助的呼吸量数据。患者使用 2 种不同的 BIPAP 呼吸机(固定 BIPAP 和灵活 BIPAP),每种呼吸机均配置为每次呼吸输送相同体积的空气(即潮气量)。灵活 BIPAP 呼吸机允许患者触发(即允许患者启动每次呼吸),而固定 BIPAP 则不允许。计算并比较特定呼吸平台(FB 或 BIPAP)之间量化潮气量变化的 session 内和 session 间指标。此外,通过口头反馈对患者对两种 BIPAP 呼吸机的耐受性进行定性评估。
两种 BIPAP 呼吸机患者均可耐受,尽管固定 BIPAP 的耐受性不如灵活 BIPAP。与 FB 相比,两种 BIPAP 呼吸机的 session 内潮气量变化均显著降低(<.05)。然而,与 FB 相比,只有固定 BIPAP 显著降低了 session 间潮气量变化。
基于潮气量与肿瘤运动之间已确立的相关性,潮气量变化的任何减少都可能导致肿瘤运动变化的减少。发现固定 BIPAP 通气患者可耐受,并且与 FB 相比,显示出显著降低 session 内和 session 间潮气量变化。因此,有必要对固定 BIPAP 的潜力进行进一步研究,以确定可能的临床益处。