Bakshi Andrew, Riaz Moeen, Orchard Suzanne G, Carr Prudence R, Joshi Amit D, Cao Yin, Rebello Richard, Nguyen-Dumont Tú, Southey Melissa C, Millar Jeremy L, Gately Lucy, Gibbs Peter, Ford Leslie G, Parnes Howard L, Chan Andrew T, McNeil John J, Lacaze Paul
Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC 3004, Australia.
Clinical and Translational Epidemiology Unit, MGH Cancer Center, Massachusetts General Hospital and Harvard Medical School, Boston, MA 02108, USA.
Cancers (Basel). 2021 Nov 19;13(22):5815. doi: 10.3390/cancers13225815.
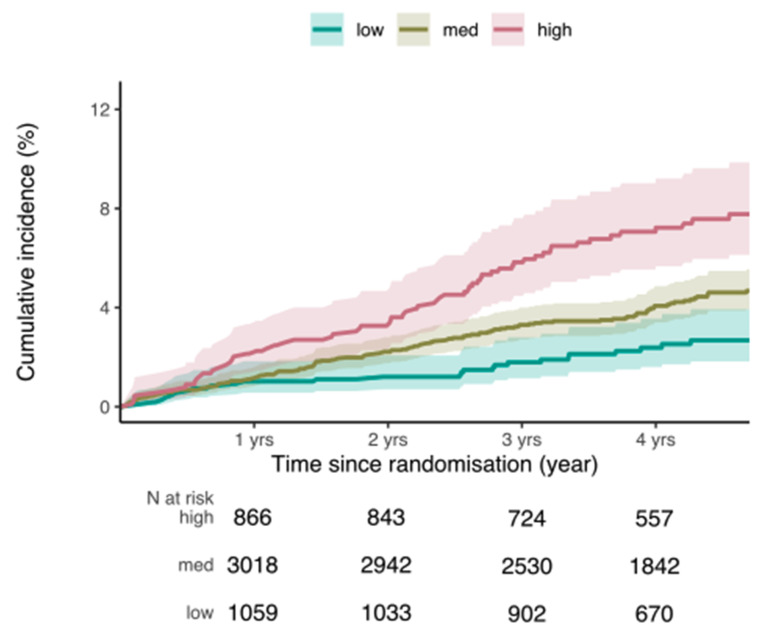
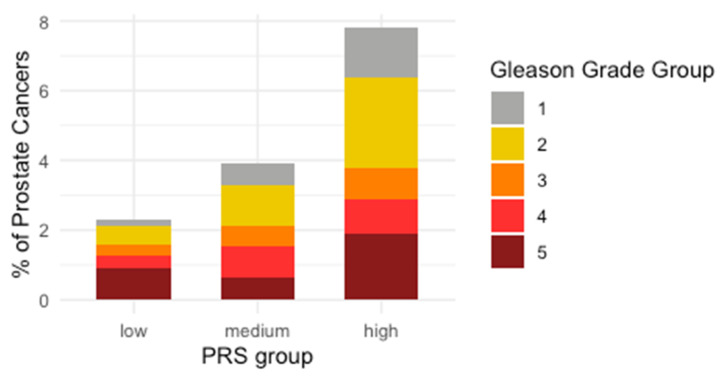
Despite the high prevalence of prostate cancer in older men, the predictive value of a polygenic risk score (PRS) remains uncertain in men aged ≥70 years. We used a 6.6 million-variant PRS to predict the risk of incident prostate cancer in a prospective study of 5701 men of European descent aged ≥70 years (mean age 75 years) enrolled in the ASPirin in Reducing Events in the Elderly (ASPREE) clinical trial. The study endpoint was prostate cancer, including metastatic or non-metastatic disease, confirmed by an expert panel. After excluding participants with a history of prostate cancer at enrolment, we used a multivariable Cox proportional hazards model to assess the association between the PRS and incident prostate cancer risk, adjusting for covariates. Additionally, we examined the distribution of Gleason grade groups by PRS group to determine if a higher PRS was associated with higher grade disease. We tested for interaction between the PRS and aspirin treatment. Logistic regression was used to independently assess the association of the PRS with prevalent (pre-trial) prostate cancer, reported in medical histories. During a median follow-up time of 4.6 years, 218 of the 5701 participants (3.8%) were diagnosed with prostate cancer. The PRS predicted incident risk with a hazard ratio (HR) of 1.52 per standard deviation (SD) (95% confidence interval (CI) 1.33-1.74, < 0.001). Men in the top quintile of the PRS distribution had an almost three times higher risk of prostate cancer than men in the lowest quintile (HR = 2.99 (95% CI 1.90-4.27), < 0.001). However, a higher PRS was not associated with a higher Gleason grade groups. We found no interaction between aspirin treatment and the PRS for prostate cancer risk. The PRS was also associated with prevalent prostate cancer (odds ratio = 1.80 per SD (95% CI 1.65-1.96), < 0.001).While a PRS for prostate cancer is strongly associated with incident risk in men aged ≥70 years, the clinical utility of the PRS as a biomarker is currently limited by its inability to select for clinically significant disease.
尽管老年男性前列腺癌的患病率很高,但多基因风险评分(PRS)在70岁及以上男性中的预测价值仍不确定。在一项针对5701名年龄≥70岁(平均年龄75岁)的欧洲裔男性的前瞻性研究中,我们使用了一个包含660万个变异的PRS来预测前列腺癌发病风险,这些男性参与了“老年人减少事件中的阿司匹林”(ASPREE)临床试验。研究终点是前列腺癌,包括转移性或非转移性疾病,由专家小组确认。在排除入组时患有前列腺癌病史的参与者后,我们使用多变量Cox比例风险模型来评估PRS与前列腺癌发病风险之间的关联,并对协变量进行调整。此外,我们按PRS组检查了 Gleason分级组的分布,以确定较高的PRS是否与更高分级的疾病相关。我们测试了PRS与阿司匹林治疗之间的相互作用。使用逻辑回归独立评估PRS与病史中报告的现患(试验前)前列腺癌的关联。在中位随访时间4.6年期间,5701名参与者中有218人(3.8%)被诊断患有前列腺癌。PRS预测发病风险,每标准差(SD)的风险比(HR)为1.52(95%置信区间(CI)1.33 - 1.74,P < 0.001)。PRS分布最高五分位数的男性患前列腺癌的风险几乎是最低五分位数男性的三倍(HR = 2.99(95%CI 1.90 - 4.27),P < 0.001)。然而,较高的PRS与较高的Gleason分级组无关。我们发现阿司匹林治疗与PRS对前列腺癌风险没有相互作用。PRS也与现患前列腺癌相关(每标准差的优势比 = 1.80(95%CI 1.65 - 1.96),P < 0.001)。虽然前列腺癌的PRS与70岁及以上男性的发病风险密切相关,但PRS作为生物标志物的临床效用目前受到其无法筛选出具有临床意义疾病的限制。