Lacaze Paul, Bakshi Andrew, Riaz Moeen, Orchard Suzanne G, Tiller Jane, Neumann Johannes T, Carr Prudence R, Joshi Amit D, Cao Yin, Warner Erica T, Manning Alisa, Nguyen-Dumont Tú, Southey Melissa C, Milne Roger L, Ford Leslie, Sebra Robert, Schadt Eric, Gately Lucy, Gibbs Peter, Thompson Bryony A, Macrae Finlay A, James Paul, Winship Ingrid, McLean Catriona, Zalcberg John R, Woods Robyn L, Chan Andrew T, Murray Anne M, McNeil John J
Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC 3004, Australia.
Clinical and Translational Epidemiology Unit, MGH Cancer Center, Massachusetts General Hospital and Harvard Medical School, Boston, MA 02108, USA.
Cancers (Basel). 2021 Jul 14;13(14):3533. doi: 10.3390/cancers13143533.
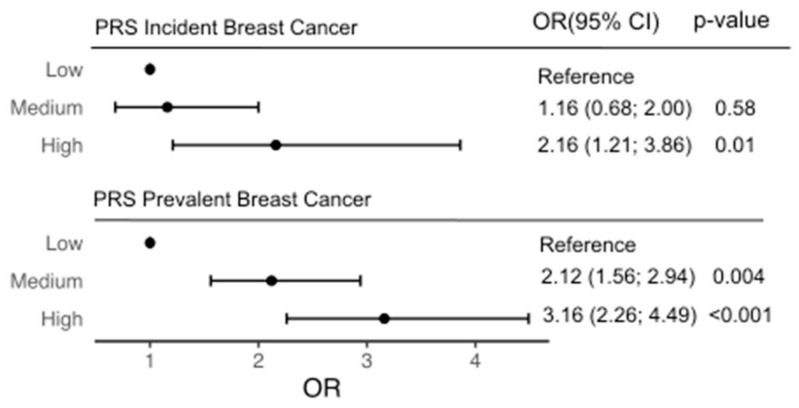
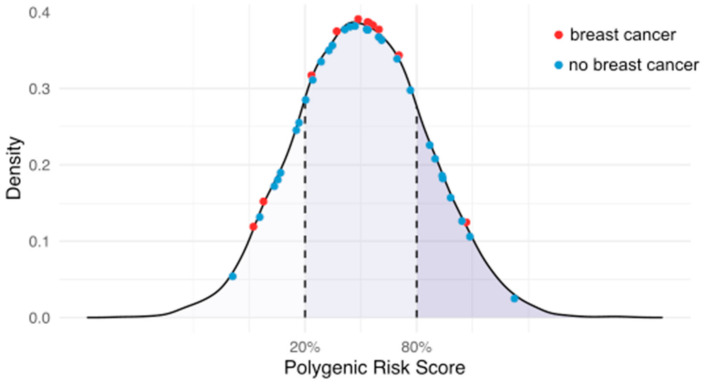
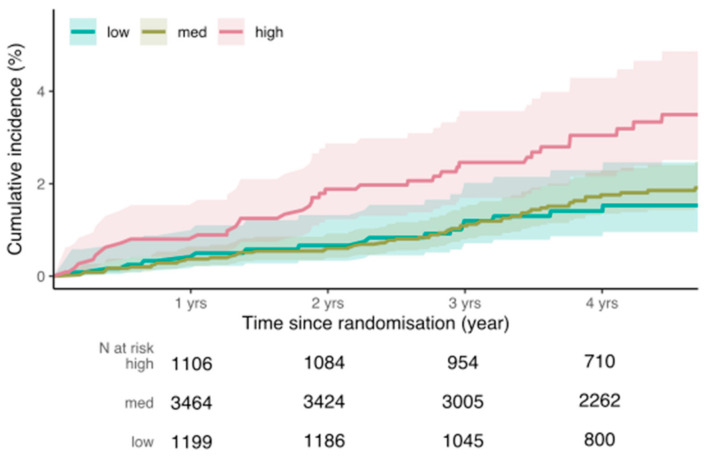
Genomic risk prediction models for breast cancer (BC) have been predominantly developed with data from women aged 40-69 years. Prospective studies of older women aged ≥70 years have been limited. We assessed the effect of a 313-variant polygenic risk score (PRS) for BC in 6339 older women aged ≥70 years (mean age 75 years) enrolled into the ASPREE trial, a randomized double-blind placebo-controlled clinical trial investigating the effect of daily 100 mg aspirin on disability-free survival. We evaluated incident BC diagnoses over a median follow-up time of 4.7 years. A multivariable Cox regression model including conventional BC risk factors was applied to prospective data, and re-evaluated after adding the PRS. We also assessed the association of rare pathogenic variants (PVs) in BC susceptibility genes (). The PRS, as a continuous variable, was an independent predictor of incident BC (hazard ratio (HR) per standard deviation (SD) = 1.4, 95% confidence interval (CI) 1.3-1.6) and hormone receptor (ER/PR)-positive disease (HR = 1.5 (CI 1.2-1.9)). Women in the top quintile of the PRS distribution had over two-fold higher risk of BC than women in the lowest quintile (HR = 2.2 (CI 1.2-3.9)). The concordance index of the model without the PRS was 0.62 (95% CI 0.56-0.68), which improved after addition of the PRS to 0.65 (95% CI 0.59-0.71). Among 41 (0.6%) carriers of PVs in BC susceptibility genes, we observed no incident BC diagnoses. Our study demonstrates that a PRS predicts incident BC risk in women aged 70 years and older, suggesting potential clinical utility extends to this older age group.
乳腺癌(BC)的基因组风险预测模型主要是基于40至69岁女性的数据开发的。对70岁及以上老年女性的前瞻性研究一直有限。我们在6339名70岁及以上(平均年龄75岁)的老年女性中评估了一种包含313个变异的乳腺癌多基因风险评分(PRS)的效果,这些女性参加了ASPREE试验,这是一项随机双盲安慰剂对照临床试验,旨在研究每日服用100毫克阿司匹林对无残疾生存期的影响。我们评估了在中位随访时间4.7年期间的乳腺癌确诊情况。将包含传统乳腺癌风险因素的多变量Cox回归模型应用于前瞻性数据,并在加入PRS后重新评估。我们还评估了乳腺癌易感基因中罕见致病变异(PVs)的关联性。作为连续变量的PRS是乳腺癌发病的独立预测因素(每标准差(SD)的风险比(HR)=1.4,95%置信区间(CI)1.3 - 1.6)以及激素受体(ER/PR)阳性疾病的独立预测因素(HR = 1.5(CI 1.2 - 1.9))。PRS分布最高五分位数的女性患乳腺癌的风险是最低五分位数女性的两倍多(HR = 2.2(CI 1.2 - 3.9))。不包含PRS的模型的一致性指数为0.62(95%CI 0.56 - 0.68),加入PRS后提高到0.65(95%CI 0.59 - 0.71)。在41名(0.6%)乳腺癌易感基因PVs携带者中,我们未观察到乳腺癌确诊病例。我们的研究表明,PRS可预测70岁及以上女性的乳腺癌发病风险,提示其潜在临床应用可扩展至该老年人群体。