Health Economics Unit, Institute of Applied Health Research, University of Birmingham, Birmingham, UK.
Institute of Applied Health Research, University of Birmingham, Birmingham, UK.
Thorax. 2022 Oct;77(10):976-986. doi: 10.1136/thoraxjnl-2021-217463. Epub 2021 Nov 26.
Chronic obstructive pulmonary disease (COPD) is a chronic disease associated with recurring exacerbations, which influence morbidity and mortality for the patient, while placing significant resource burdens on healthcare systems. Non-invasive ventilation (NIV) in a domiciliary setting can help prevent admissions, but the economic evidence to support NIV use is limited.
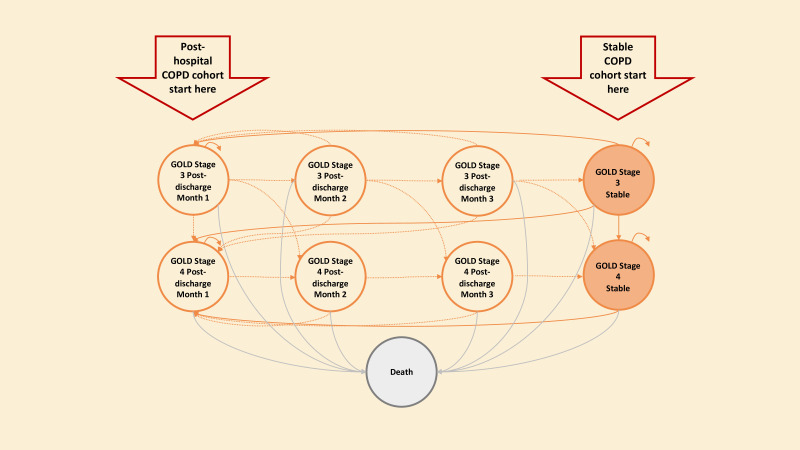
A Markov model-based cost-utility analysis from the UK National Health Service perspective compared the cost-effectiveness of domiciliary NIV with usual care for two end-stage COPD populations; a stable COPD population commencing treatment with no recent hospital admission; and a posthospital population starting treatment following admission to hospital for an exacerbation. Hospitalisation rates in patients receiving domiciliary NIV compared with usual care were derived from randomised controlled studies in a recent systematic review. Other model parameters were updated with recent evidence.
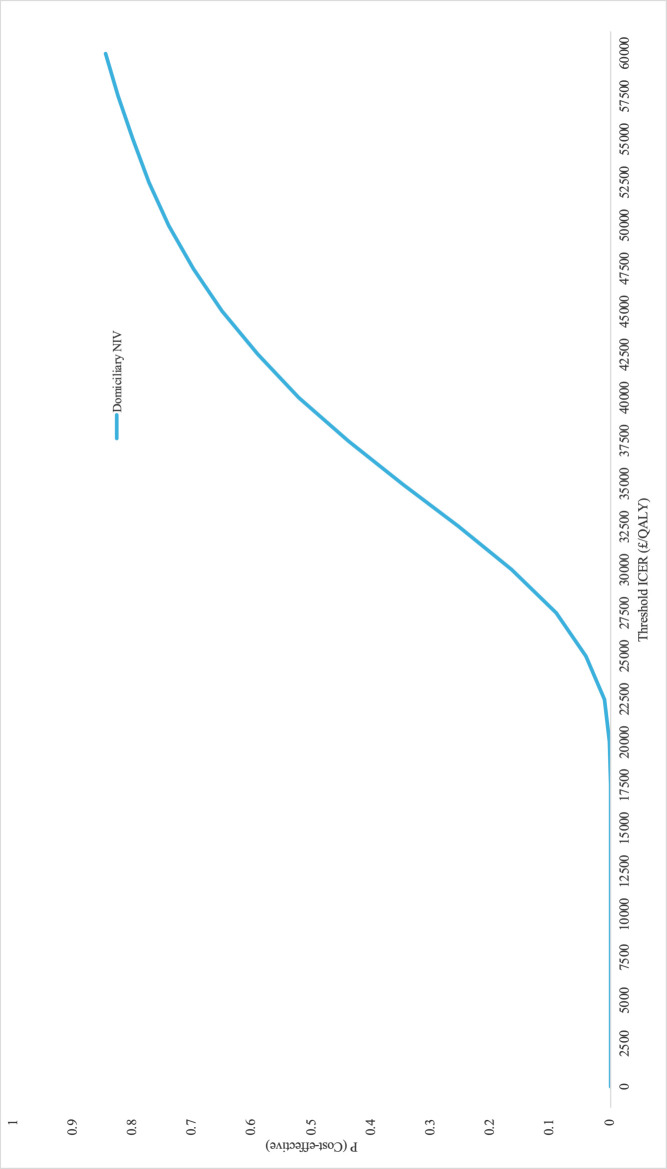
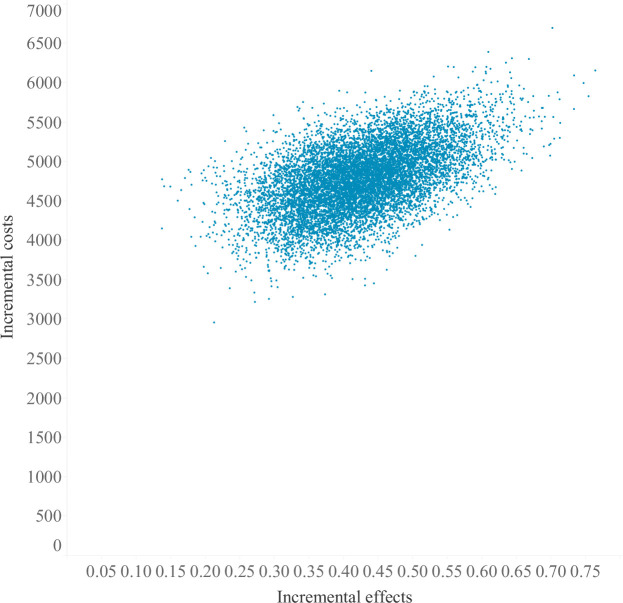
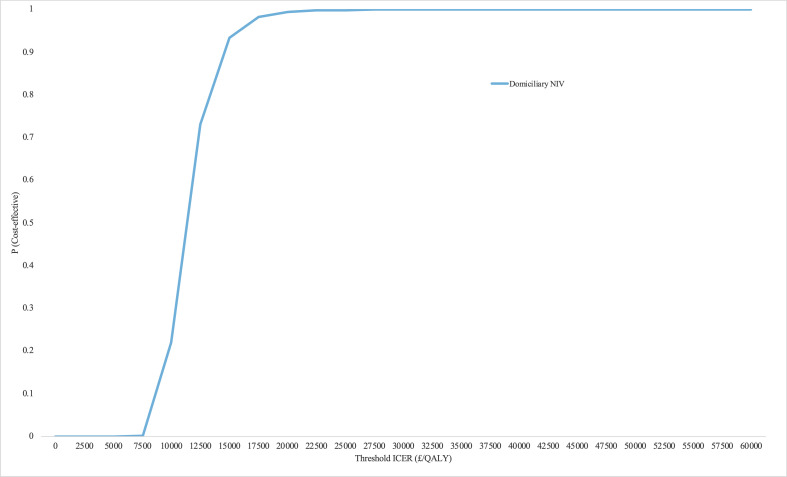
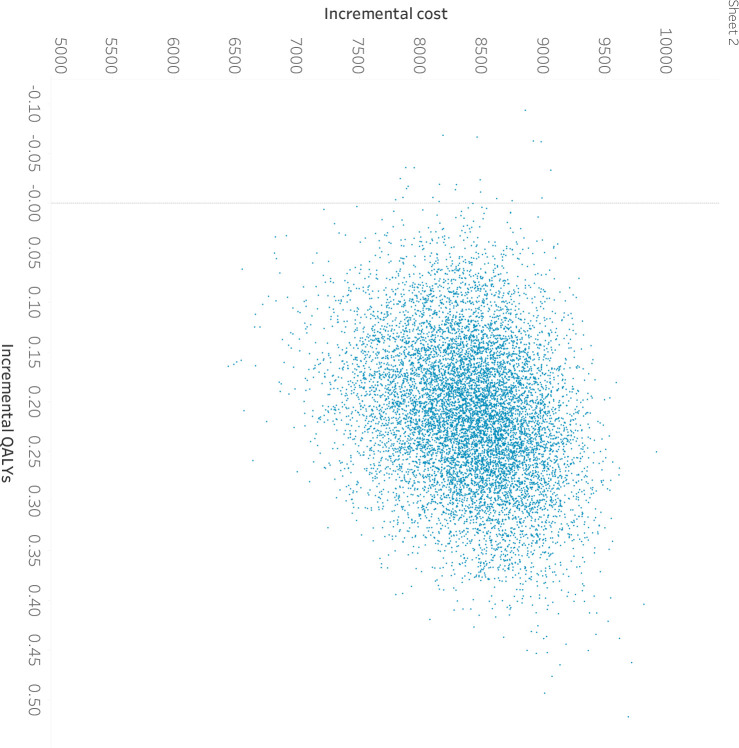
At the threshold of £20 000 per quality-adjusted life-year (QALY) domiciliary NIV is 99.9% likely cost-effective in a posthospital population, but unlikely (4%) to be cost-effective in stable populations. The incremental cost-effective ratio (ICER) was £11 318/QALY gained in the posthospital population and £27 380/QALY gained in the stable population. Cost-effectiveness estimates were sensitive to longer-term readmission and mortality risks, and duration of benefit from NIV. Indeed, for stable Global Initiative for Chronic Obstructive Lung Disease (GOLD) for stage 4 patients, or with higher mortality and exacerbation risks, ICERs were close to the £20 000/QALY threshold.
Domiciliary NIV is likely cost-effective for posthospitalised patients, with uncertainty around the cost-effectiveness of domiciliary NIV in stable patients with COPD on which further research should focus.
慢性阻塞性肺疾病(COPD)是一种与反复发作相关的慢性疾病,会影响患者的发病率和死亡率,同时给医疗系统带来巨大的资源负担。家庭环境中的无创通气(NIV)可以帮助预防住院,但支持 NIV 使用的经济证据有限。
从英国国家医疗服务体系的角度出发,采用基于马尔可夫模型的成本效用分析,比较了家庭 NIV 与常规护理在两种终末期 COPD 人群中的成本效益:无近期住院史的稳定 COPD 人群开始治疗;因 COPD 加重而住院后开始治疗的住院人群。家庭 NIV 组和常规护理组的住院率是从最近一项系统评价的随机对照研究中得出的。其他模型参数根据最新证据进行了更新。
在 20000 英镑/QALY 的阈值下,家庭 NIV 在住院后人群中具有 99.9%的成本效益可能性,但在稳定人群中不太可能(4%)具有成本效益。在住院后人群中,增量成本效益比(ICER)为 11318 英镑/QALY,在稳定人群中为 27380 英镑/QALY。成本效益估计对长期再入院和死亡率风险以及 NIV 获益的持续时间敏感。实际上,对于稳定的全球慢性阻塞性肺疾病倡议(GOLD)第 4 阶段患者,或死亡率和加重风险较高的患者,ICER 接近 20000 英镑/QALY 的阈值。
家庭 NIV 可能对住院后患者具有成本效益,但对 COPD 稳定患者的家庭 NIV 的成本效益存在不确定性,应进一步研究。