Dretzke Janine, Moore David, Dave Chirag, Mukherjee Rahul, Price Malcolm J, Bayliss Sue, Wu Xiaoying, Jordan Rachel E, Turner Alice M
Institute of Applied Health Research, College of Medical and Dental Sciences, University of Birmingham, Edgbaston.
Heart of England NHS Foundation Trust, Heartlands Hospital.
Int J Chron Obstruct Pulmon Dis. 2016 Sep 16;11:2269-2286. doi: 10.2147/COPD.S104238. eCollection 2016.
Noninvasive ventilation (NIV) improves survival among patients with hypercapnic respiratory failure in hospital, but evidence for its use in domiciliary settings is limited. A patient's underlying risk of having an exacerbation may affect any potential benefit that can be gained from domiciliary NIV. This is the first comprehensive systematic review to stratify patients based on a proxy for exacerbation risk: patients in a stable state and those immediately post-exacerbation hospitalization.
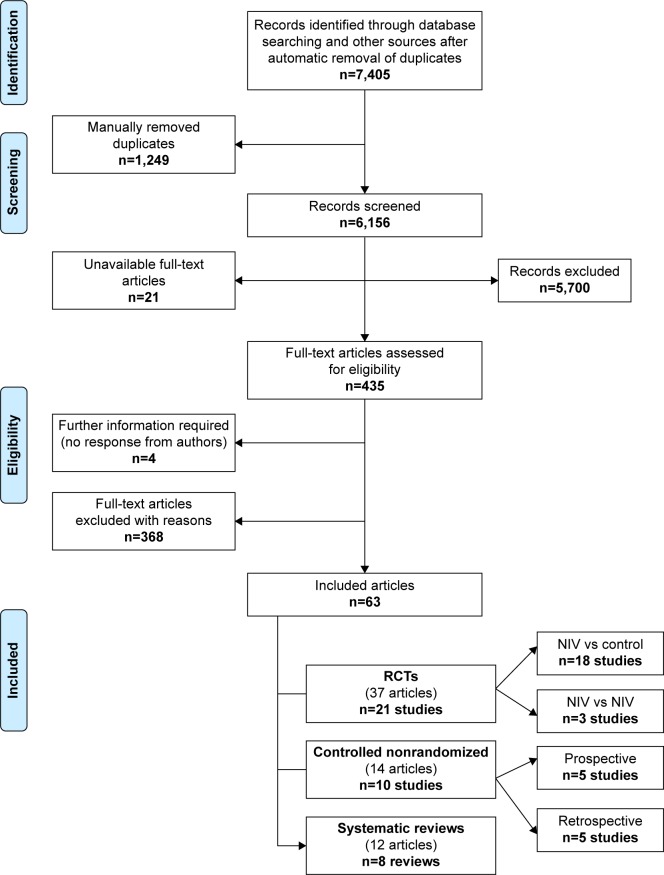
A systematic review of nonrandomized and randomized controlled trials (RCTs) was undertaken in order to compare the relative effectiveness of different types of domiciliary NIV and usual care on hospital admissions, mortality, and health-related quality of life. Standard systematic review methods were used for identifying studies (until September 2014), quality appraisal, and synthesis. Data were presented in forest plots and pooled where appropriate using random-effects meta-analysis.
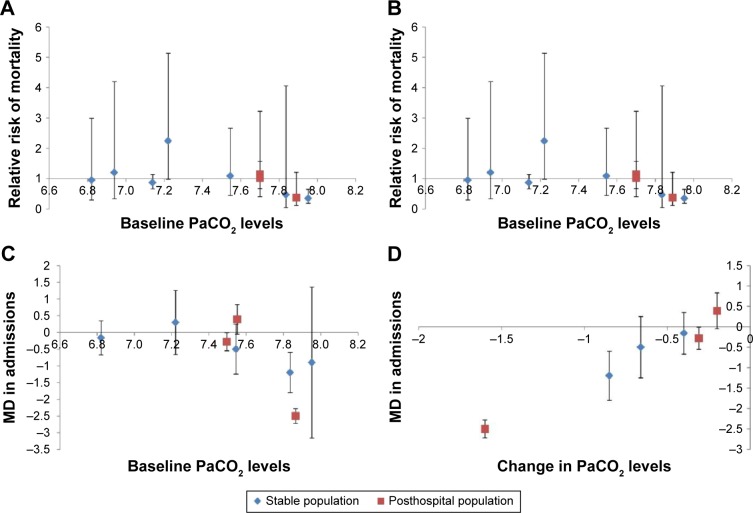
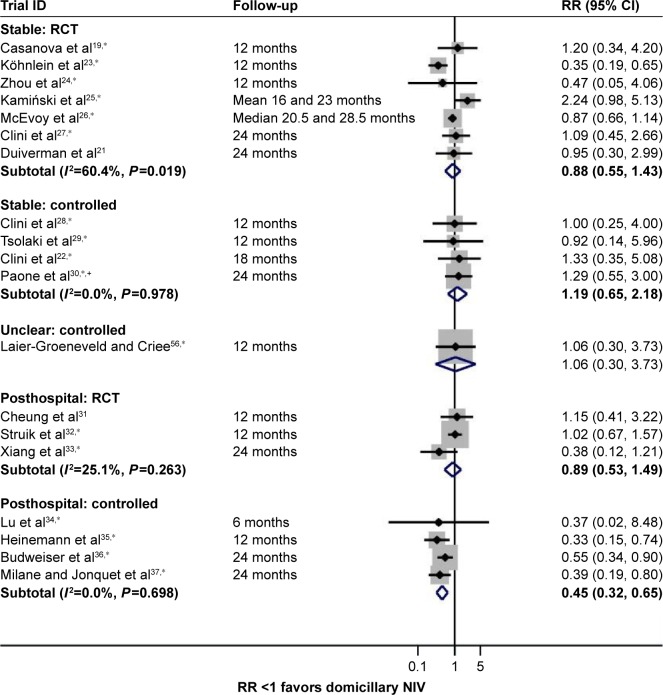
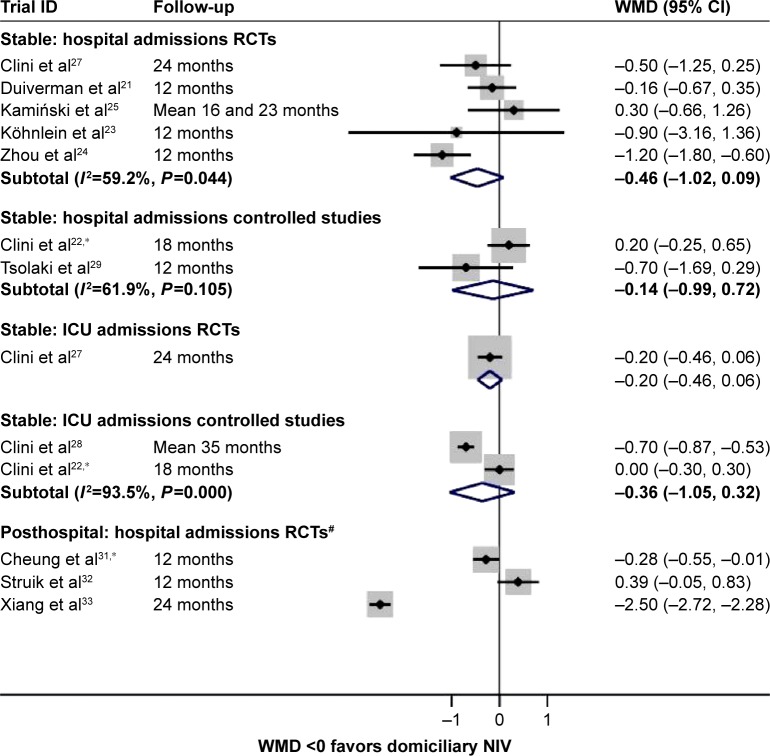
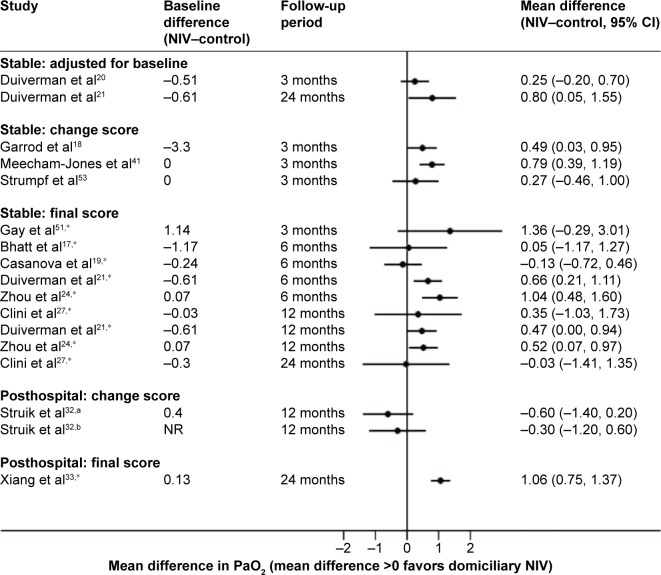
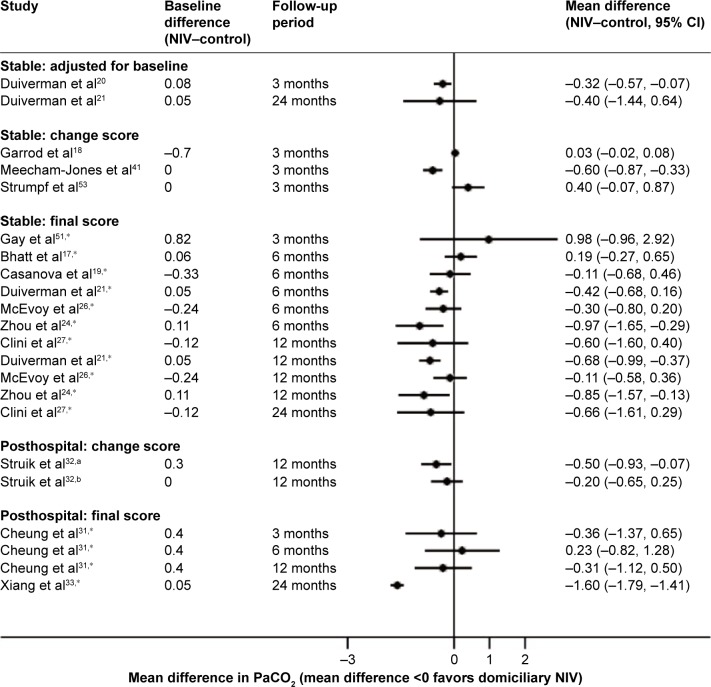
Thirty-one studies were included. For stable patients, there was no evidence of a survival benefit from NIV (relative risk [RR] 0.88 [0.55, 1.43], =60.4%, n=7 RCTs), but there was a possible trend toward fewer hospitalizations (weighted mean difference -0.46 [-1.02, 0.09], =59.2%, n=5 RCTs) and improved health-related quality of life. For posthospital patients, survival benefit could not be demonstrated within the three RCTs (RR 0.89 [0.53, 1.49], =25.1%), although there was evidence of benefit from four non-RCTs (RR 0.45 [0.32, 0.65], =0%). Effects on hospitalizations were inconsistent. Post hoc analyses suggested that NIV-related improvements in hypercapnia were associated with reduced hospital admissions across both populations. Little data were available comparing different types of NIV.
The effectiveness of domiciliary NIV remains uncertain; however, some patients may benefit. Further research is required to identify these patients and to explore the relevance of improvements in hypercapnia in influencing clinical outcomes. Optimum time points for commencing domiciliary NIV and equipment settings need to be established.
无创通气(NIV)可提高医院内高碳酸血症呼吸衰竭患者的生存率,但在家居环境中使用NIV的证据有限。患者病情加重的潜在风险可能会影响从家庭无创通气中获得的任何潜在益处。这是第一项基于病情加重风险指标对患者进行分层的全面系统评价:病情稳定的患者和病情加重后刚出院的患者。
对非随机和随机对照试验(RCT)进行系统评价,以比较不同类型的家庭无创通气与常规治疗在住院、死亡率和健康相关生活质量方面的相对有效性。采用标准的系统评价方法来识别研究(截至2014年9月)、质量评估和综合分析。数据以森林图呈现,并在适当情况下使用随机效应荟萃分析进行汇总。
纳入31项研究。对于病情稳定的患者,没有证据表明无创通气能带来生存获益(相对危险度[RR]0.88[0.55,1.43],I²=60.4%,n=7项RCT),但住院次数可能有减少的趋势(加权平均差-0.46[-1.02,0.09],I²=59.2%,n=5项RCT),且健康相关生活质量有所改善。对于出院后的患者,在3项RCT中未显示出生存获益(RR 0.89[0.53,1.49],I²=25.1%),尽管4项非RCT有获益证据(RR 0.45[0.32,0.65],I²=0%)。对住院次数影响不一致。事后分析表明,无创通气相关的高碳酸血症改善与两组患者住院次数减少有关。比较不同类型无创通气的数据很少。
家庭无创通气的有效性仍不确定;然而,一些患者可能会从中获益。需要进一步研究以识别这些患者,并探讨高碳酸血症改善对临床结局影响的相关性。需要确定开始家庭无创通气的最佳时间点和设备设置。