Department of Child and Adolescent Psychiatry and Psychotherapy, Psychiatric University Hospital Zurich, University of Zurich, Zurich, Switzerland.
The Zurich Program for Sustainable Development of Mental Health Services (ZInEP), Psychiatric University Hospital Zurich, Zurich, Switzerland.
Transl Psychiatry. 2021 Nov 26;11(1):600. doi: 10.1038/s41398-021-01720-0.
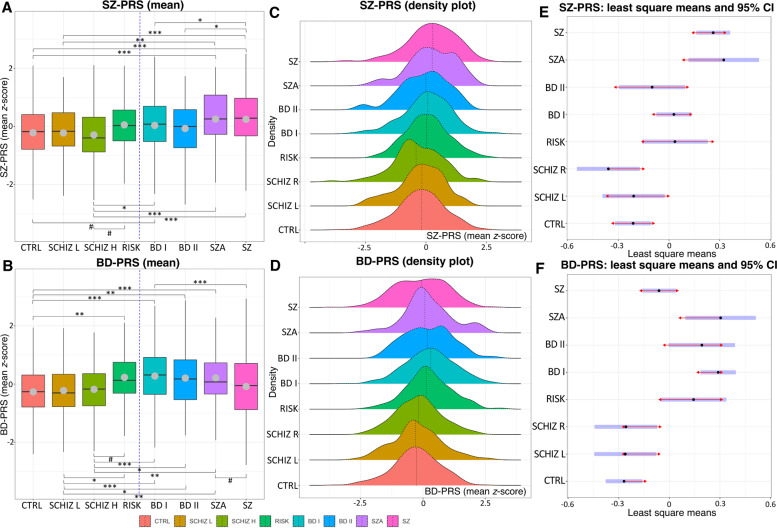
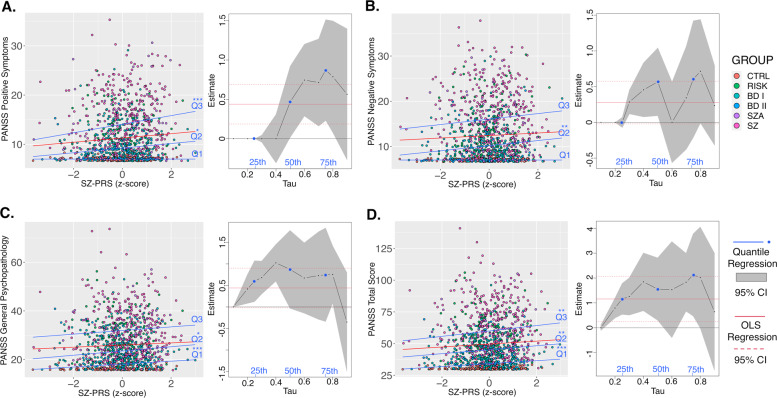
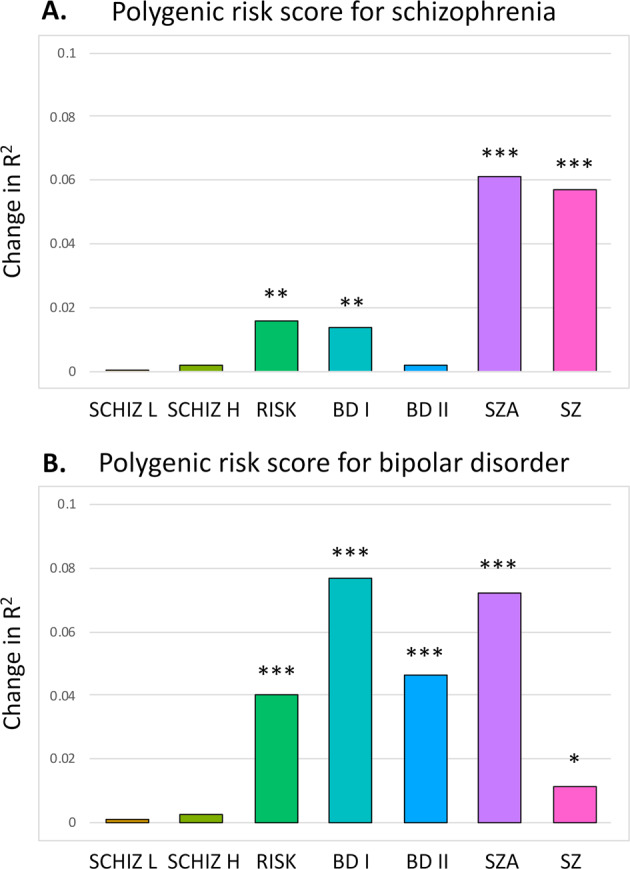
As early detection of symptoms in the subclinical to clinical psychosis spectrum may improve health outcomes, knowing the probabilistic susceptibility of developing a disorder could guide mitigation measures and clinical intervention. In this context, polygenic risk scores (PRSs) quantifying the additive effects of multiple common genetic variants hold the potential to predict complex diseases and index severity gradients. PRSs for schizophrenia (SZ) and bipolar disorder (BD) were computed using Bayesian regression and continuous shrinkage priors based on the latest SZ and BD genome-wide association studies (Psychiatric Genomics Consortium, third release). Eight well-phenotyped groups (n = 1580; 56% males) were assessed: control (n = 305), lower (n = 117) and higher (n = 113) schizotypy (both groups of healthy individuals), at-risk for psychosis (n = 120), BD type-I (n = 359), BD type-II (n = 96), schizoaffective disorder (n = 86), and SZ groups (n = 384). PRS differences were investigated for binary traits and the quantitative Positive and Negative Syndrome Scale. Both BD-PRS and SZ-PRS significantly differentiated controls from at-risk and clinical groups (Nagelkerke's pseudo-R: 1.3-7.7%), except for BD type-II for SZ-PRS. Out of 28 pairwise comparisons for SZ-PRS and BD-PRS, 9 and 12, respectively, reached the Bonferroni-corrected significance. BD-PRS differed between control and at-risk groups, but not between at-risk and BD type-I groups. There was no difference between controls and schizotypy. SZ-PRSs, but not BD-PRSs, were positively associated with transdiagnostic symptomology. Overall, PRSs support the continuum model across the psychosis spectrum at the genomic level with possible irregularities for schizotypy. The at-risk state demands heightened clinical attention and research addressing symptom course specifiers. Continued efforts are needed to refine the diagnostic and prognostic accuracy of PRSs in mental healthcare.
由于在亚临床至临床精神病谱系中早期发现症状可能会改善健康结果,因此了解发生疾病的概率易感性可以指导缓解措施和临床干预。在这种情况下,量化多个常见遗传变异的加性效应的多基因风险评分 (PRS) 有可能预测复杂疾病并指示严重程度梯度。使用贝叶斯回归和基于最新的精神分裂症和双相情感障碍全基因组关联研究 (精神疾病基因组学联盟,第三版) 的连续收缩先验,计算了精神分裂症 (SZ) 和双相情感障碍 (BD) 的 PRS。评估了八个表型良好的组 (n=1580; 56%为男性):对照组 (n=305)、较低 (n=117) 和较高 (n=113) 精神分裂症倾向 (两组均为健康个体)、精神病风险 (n=120)、BD 型-I (n=359)、BD 型-II (n=96)、分裂情感障碍 (n=86) 和 SZ 组 (n=384)。研究了二元特征和定量阳性和阴性综合征量表的 PRS 差异。BD-PRS 和 SZ-PRS 均显着区分了对照组与高危和临床组 (Nagelkerke 的伪 R:1.3-7.7%),BD 型-II 除外。在 28 项 SZ-PRS 和 BD-PRS 的成对比较中,分别有 9 项和 12 项达到了 Bonferroni 校正的显着性。BD-PRS 在对照组和高危组之间存在差异,但在高危组和 BD 型-I 组之间没有差异。对照组与精神分裂症倾向之间没有差异。SZ-PRS,但不是 BD-PRS,与跨诊断症状学呈正相关。总体而言,PRS 从基因组水平上支持精神病谱的连续模型,可能在精神分裂症倾向方面存在不规则性。高危状态需要高度的临床关注和研究,以解决症状过程的特征。需要继续努力提高 PRS 在精神保健中的诊断和预后准确性。