Clinic for Orthopedics and Trauma Surgery, Center for Orthopedics, Trauma Surgery and Spinal Cord Injury, Heidelberg University Hospital, Schlierbacher Landstrasse 200a, 69118, Heidelberg, Germany.
Clinic for Orthopedics and Traumatology, University Medical Center Schleswig-Holstein, Campus Kiel, Kiel, Germany.
Arch Orthop Trauma Surg. 2022 Dec;142(12):4041-4054. doi: 10.1007/s00402-021-04274-4. Epub 2021 Dec 1.
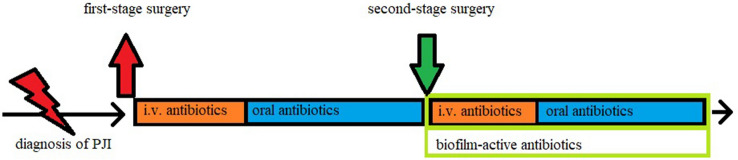
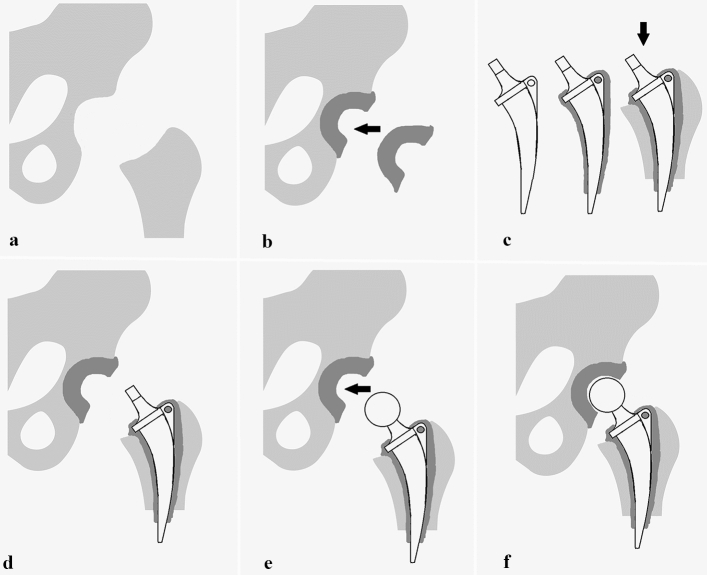
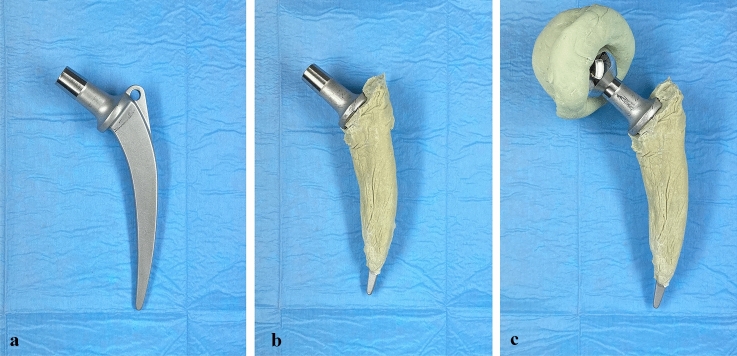
Two-stage revision remains the gold standard treatment for most chronically infected and complex total hip arthroplasty infections. To improve patient outcome and reduce complication rates, we have developed a novel custom-made articulating hip spacer technique and present our short-term results.
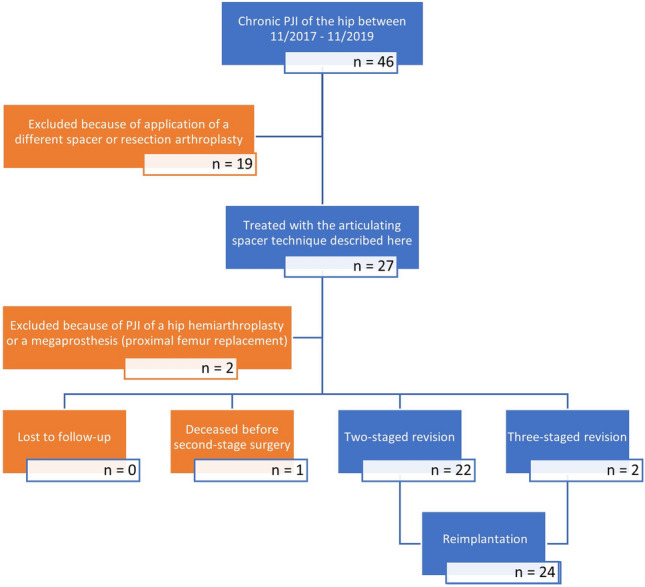
Between November 2017 and November 2019, 27 patients (mean age 70 years) underwent two-stage revision for periprosthetic joint infection of the hip using the articulating spacer design described here. We retrospectively analyzed spacer-related complications as well as rates for complication, infection control, and implant survivorship after final reimplantation. Furthermore, we prospectively collected patient-reported health-related quality of life (HRQoL) scores prior to spacer implantation, with the spacer and after reimplantation of the new prosthesis.
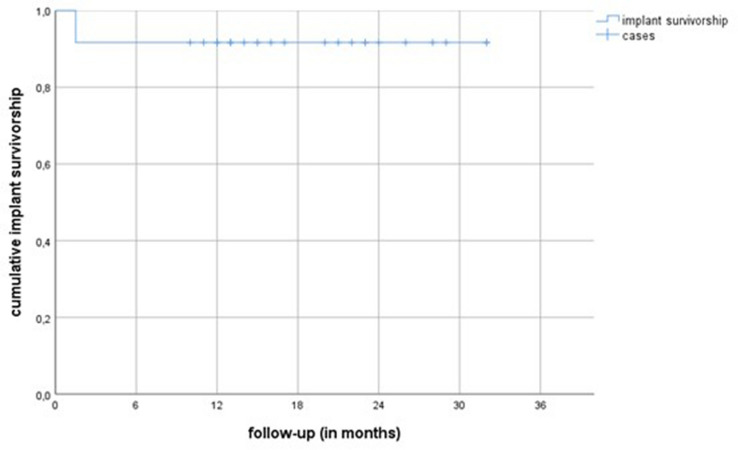
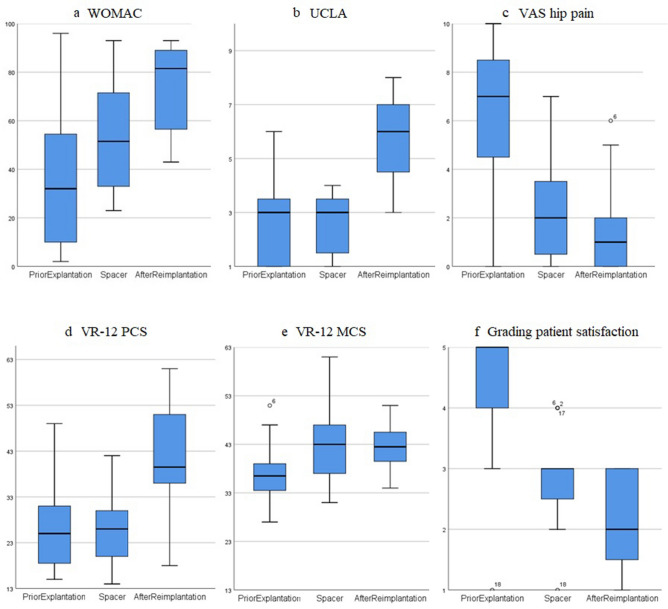
An additional round of spacer exchange was performed in two patients (8.3%), persistent wound discharge was the reason in both cases. We had one (4.2%) spacer-related mechanical complication, a dislocation that was treated with closed reduction. After reimplantation, infection control was achieved in 96% with an implant survivorship of 92% after a mean follow-up time of 19 (range 7-32, SD 7.2) months. While the scores for VR-12 MCS, VAS hip pain and patient-reported overall satisfaction significantly improved after first stage surgery, the scores for WOMAC, UCLA and VR-12 PCS significantly improved after second stage surgery.
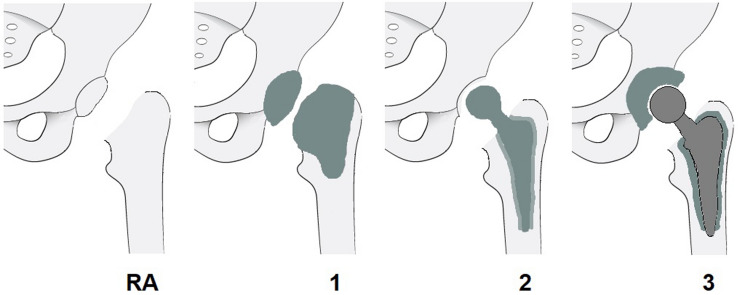
Our two-stage approach for periprosthetic joint infection shows high infection eradication and implant survivorship rates at short-term follow-up. Spacer-related complication rates were low, and we achieved high patient satisfaction rates and low pain levels already during the spacer period. To further simplify comparison between different spacer designs, we propose a new hip spacer classification system.
对于大多数慢性感染和复杂的全髋关节置换感染,两期翻修仍然是金标准治疗方法。为了改善患者的预后并降低并发症发生率,我们开发了一种新型定制关节活动髋关节 spacer 技术,并介绍了我们的短期结果。
2017 年 11 月至 2019 年 11 月,27 例(平均年龄 70 岁)患者因髋关节假体周围关节感染接受两期翻修,采用本文所述的关节活动 spacer 设计。我们回顾性分析了 spacer 相关并发症,以及最终再植入后的并发症控制、感染控制和植入物存活率。此外,我们前瞻性地收集了 spacer 植入前、植入时和新假体植入后的患者报告的健康相关生活质量(HRQoL)评分。
两名患者(8.3%)需要进行一轮 spacer 更换,这两名患者的原因都是持续性伤口渗液。我们有一例(4.2%)与 spacer 相关的机械并发症,是一例脱位,通过闭合复位治疗。再植入后,96%的患者感染得到控制,平均随访时间为 19 个月(范围 7-32,SD 7.2),植入物存活率为 92%。虽然 VR-12 MCS、VAS 髋关节疼痛和患者报告的总体满意度评分在第一阶段手术后显著改善,但 WOMAC、UCLA 和 VR-12 PCS 评分在第二阶段手术后显著改善。
我们的两期治疗方案在短期随访中显示出高的感染清除率和植入物存活率。Spacer 相关并发症发生率低,在 spacer 期间患者满意度高,疼痛水平低。为了进一步简化不同 spacer 设计之间的比较,我们提出了一种新的髋关节 spacer 分类系统。