Teoh Seth En, Masuda Yoshio, Tan Darren Jun Hao, Liu Nan, Morrison Laurie J, Ong Marcus Eng Hock, Blewer Audrey L, Ho Andrew Fu Wah
Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore.
Centre for Quantitative Medicine, Duke-NUS Medical School, Singapore, Singapore.
Ann Intensive Care. 2021 Dec 7;11(1):169. doi: 10.1186/s13613-021-00957-8.
The coronavirus disease 2019 (COVID-19) pandemic has significantly influenced epidemiology, yet its impact on out-of-hospital cardiac arrest (OHCA) remains unclear. We aimed to evaluate the impact of the pandemic on the incidence and case fatality rate (CFR) of OHCA. We also evaluated the impact on intermediate outcomes and clinical characteristics.
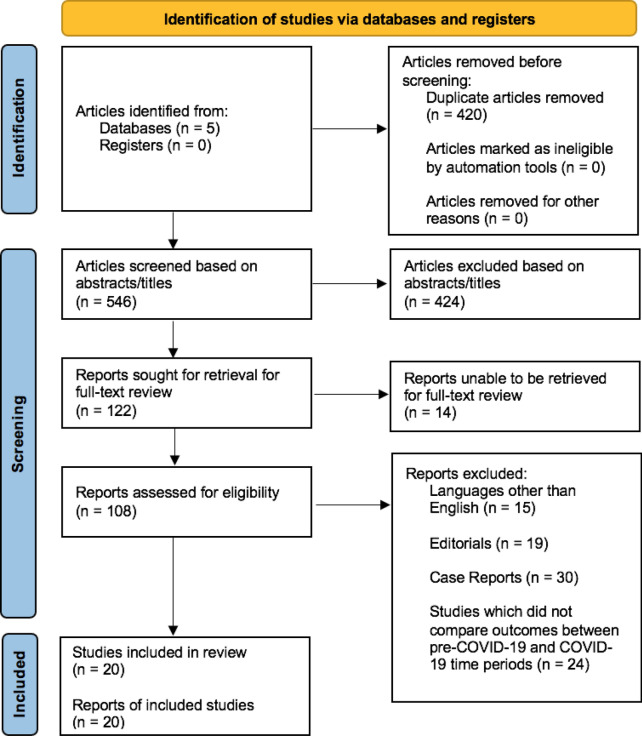
PubMed, EMBASE, Web of Science, Scopus, and Cochrane Library databases were searched from inception to May 3, 2021. Studies were included if they compared OHCA processes and outcomes between the pandemic and historical control time periods. Meta-analyses were performed for primary outcomes [annual incidence, mortality, and case fatality rate (CFR)], secondary outcomes [field termination of resuscitation (TOR), return of spontaneous circulation (ROSC), survival to hospital admission, and survival to hospital discharge], and clinical characteristics (shockable rhythm and etiologies). This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42021253879).
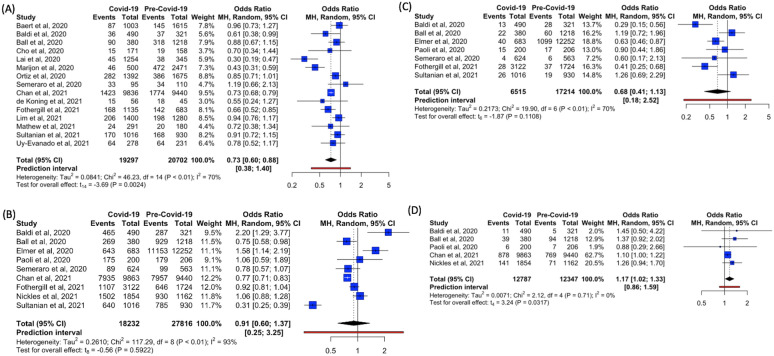
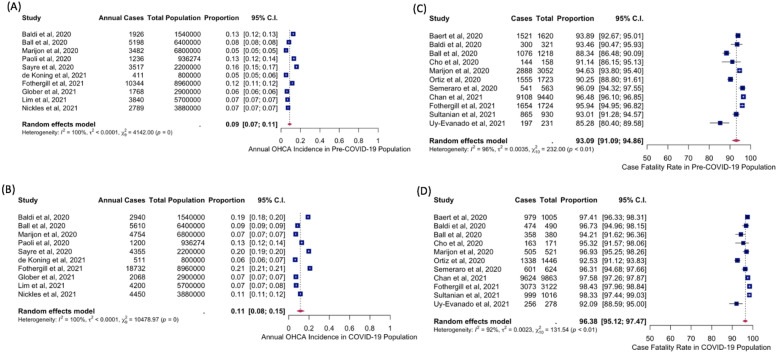
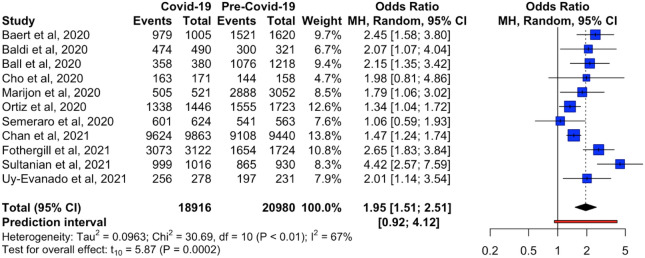
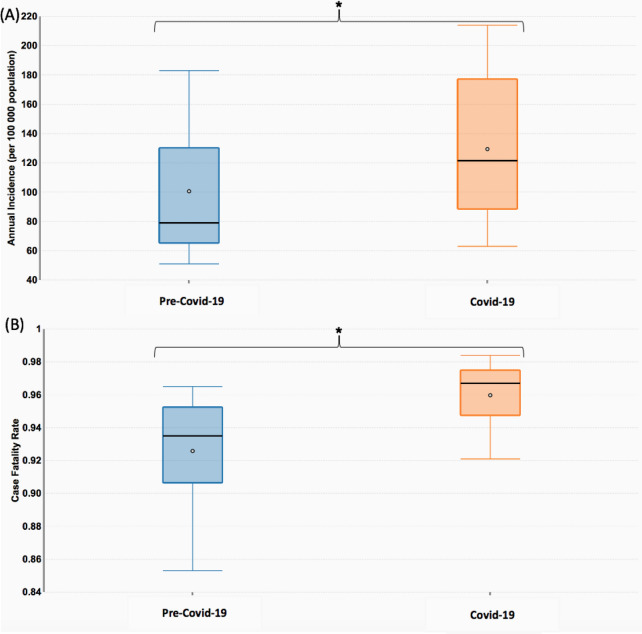
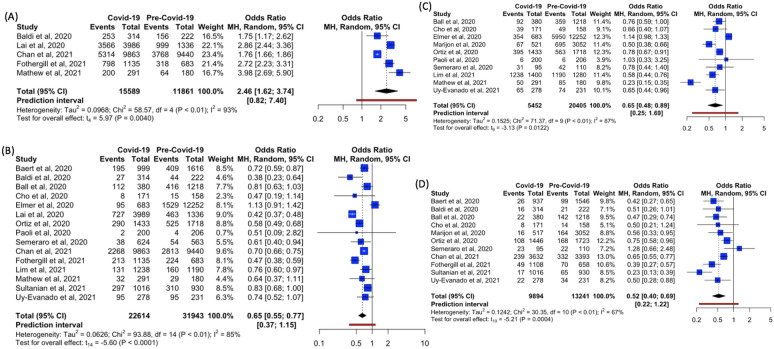
The COVID-19 pandemic was associated with a 39.5% increase in pooled annual OHCA incidence (p < 0.001). Pooled CFR was increased by 2.65% (p < 0.001), with a pooled odds ratio (OR) of 1.95 for mortality [95% confidence interval (95%CI) 1.51-2.51]. There was increased field TOR (OR = 2.46, 95%CI 1.62-3.74). There were decreased ROSC (OR = 0.65, 95%CI 0.55-0.77), survival to hospital admission (OR = 0.65, 95%CI 0.48-0.89), and survival to discharge (OR = 0.52, 95%CI 0.40-0.69). There was decreased shockable rhythm (OR = 0.73, 95%CI 0.60-0.88) and increased asphyxial etiology of OHCA (OR = 1.17, 95%CI 1.02-1.33).
Compared to the pre-pandemic period, the COVID-19 pandemic period was significantly associated with increased OHCA incidence and worse outcomes.
2019年冠状病毒病(COVID-19)大流行对流行病学产生了重大影响,但其对院外心脏骤停(OHCA)的影响仍不清楚。我们旨在评估大流行对OHCA发病率和病死率(CFR)的影响。我们还评估了对中间结局和临床特征的影响。
检索了PubMed、EMBASE、Web of Science、Scopus和Cochrane图书馆数据库,检索时间从数据库建立至2021年5月3日。纳入比较大流行时期与历史对照时期OHCA过程和结局的研究。对主要结局[年发病率、死亡率和病死率(CFR)]、次要结局[现场终止复苏(TOR)、自主循环恢复(ROSC)、入院存活和出院存活]以及临床特征(可电击心律和病因)进行荟萃分析。本研究已在国际系统评价前瞻性注册库(PROSPERO)注册(CRD42021253879)。
COVID-19大流行与汇总的年度OHCA发病率增加39.5%相关(p<0.001)。汇总的CFR增加了2.65%(p<0.001),死亡率的汇总比值比(OR)为1.95[95%置信区间(95%CI)1.51-2.51]。现场TOR增加(OR = 2.46,95%CI 1.62-3.74)。ROSC降低(OR = 0.65,95%CI 0.55-0.77),入院存活(OR = 0.65,95%CI 0.48-0.89)和出院存活降低(OR = 0.52,95%CI 0.40-0.69)。可电击心律降低(OR = 0.73,95%CI 0.60-0.88),OHCA的窒息病因增加(OR = 1.17,95%CI 1.02-1.33)。
与大流行前时期相比,COVID-19大流行时期与OHCA发病率增加和结局更差显著相关。