Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK
NIHR Oxford Biomedical Research Centre, Oxford University Hospitals NHS Foundation Trust, Oxford, UK.
BMJ Open. 2021 Dec 7;11(12):e050757. doi: 10.1136/bmjopen-2021-050757.
Observational studies have suggested a beneficial effect of taking statins on frequency of chronic obstructive pulmonary disease (COPD) exacerbations. However, clinical trials of statins in people with COPD did not confirm those results. This study aimed to investigate this association using a methodological approach, which reduces the biases associated with some previous observational study designs.
Retrospective cohort study comparing new-users of statins with non-users.
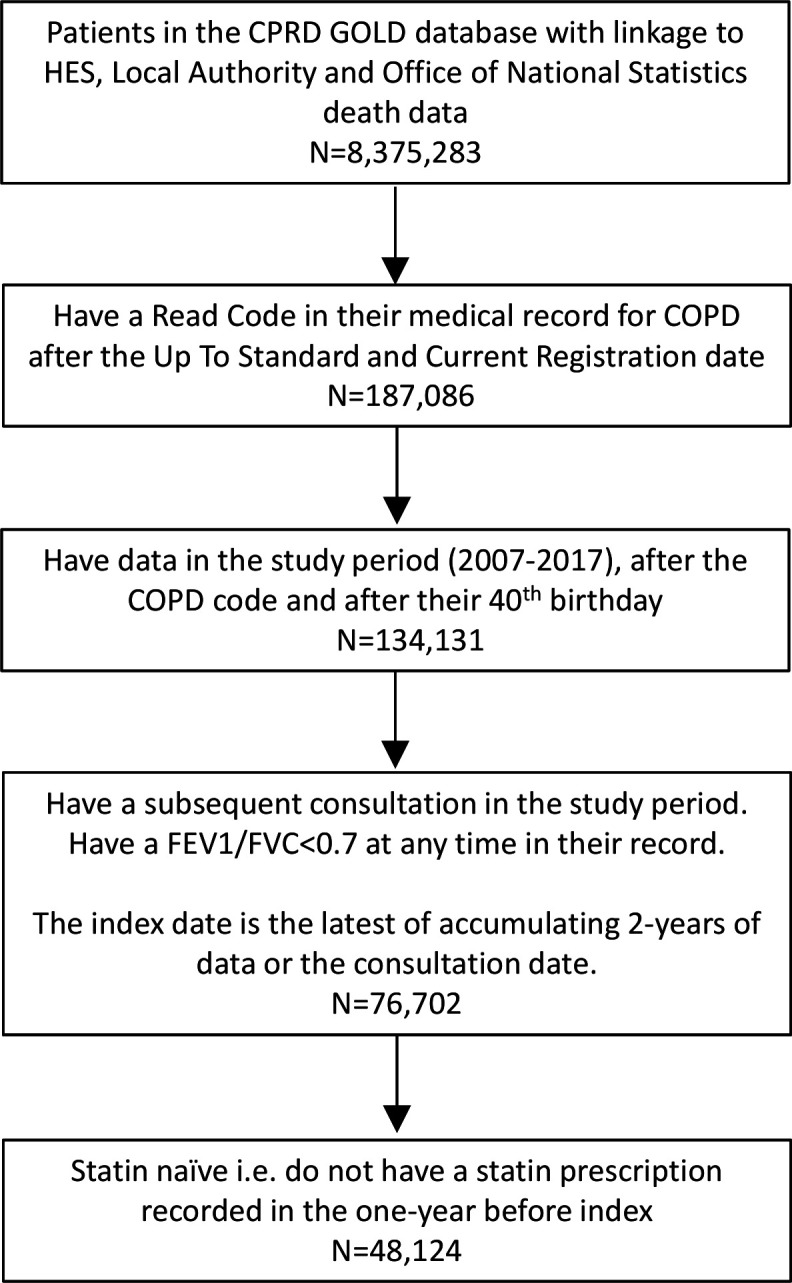
General practices in England contributing to the Clinical Practice Research Datalink in 2007-2017, with linkage to data on Hospital Episode Statistics inpatient episodes.
48 124 people with COPD, aged over 40 years, who had not been prescribed statin in the previous year.
Participants became new-users of statins at their first prescription for a statin during follow-up. They were then assumed to remain statin users. Statin users were compared with non-users.
Primary outcomes were COPD exacerbation, or severe exacerbation requiring hospitalisation. Secondary outcomes were death from any cause (for comparison with other studies) and urinary tract infection (negative-control). Maximum follow-up was 3 years. Adjusted HR were calculated using time-dependent Cox regression. The Andersen-Gill model was used for recurrent exacerbations. Covariates included demographic variables, variables related to COPD severity, cardiovascular comorbidities as time-dependent variables, and other comorbidities at baseline.
7266 participants became new-users of statins over an average 2.5 years of follow-up. In total, 30 961 people developed an exacerbation, 8110 severe exacerbation, 3650 urinary tract infection and 5355 died. Adjusted HR (95% CI) in statin users compared with non-users were first exacerbation 1.01 (0.96-1.06), severe exacerbation 0.92 (0.84-0.99), number of exacerbations 1.00 (0.97-1.04), urinary tract infection 1.10 (0.98-1.23) and death 0.63 (0.57-0.70).
In this study of health records from a Primary Care database, statin use in people with COPD was not associated with a lower risk of COPD exacerbation.
观察性研究表明,服用他汀类药物可降低慢性阻塞性肺疾病(COPD)加重的频率。然而,COPD 患者他汀类药物的临床试验并未证实这些结果。本研究旨在采用一种方法学方法来研究这种关联,该方法可以降低与某些先前观察性研究设计相关的偏倚。
比较新使用他汀类药物的患者和未使用者的回顾性队列研究。
2007 年至 2017 年期间,参与英格兰临床实践研究数据链接的普通诊所,并与医院入院统计住院患者数据链接。
48124 名年龄在 40 岁以上且在前一年未开他汀类药物的 COPD 患者。
参与者在随访期间首次开具他汀类药物处方时成为新的他汀类药物使用者。然后假定他们继续使用他汀类药物。将他汀类药物使用者与未使用者进行比较。
主要结局为 COPD 加重或需要住院治疗的严重加重。次要结局为任何原因的死亡(与其他研究比较)和尿路感染(阴性对照)。最长随访时间为 3 年。使用时间依赖性 Cox 回归计算调整后的 HR。使用 Andersen-Gill 模型进行复发性加重。协变量包括人口统计学变量、与 COPD 严重程度相关的变量、心血管合并症作为时间依赖性变量以及基线时的其他合并症。
平均随访 2.5 年后,7266 名参与者开始使用他汀类药物。共有 30961 人发生加重,8110 人发生严重加重,3650 人发生尿路感染,5355 人死亡。与未使用者相比,他汀类药物使用者的调整后 HR(95%CI)分别为首次加重 1.01(0.96-1.06)、严重加重 0.92(0.84-0.99)、加重次数 1.00(0.97-1.04)、尿路感染 1.10(0.98-1.23)和死亡 0.63(0.57-0.70)。
在这项来自初级保健数据库的健康记录研究中,COPD 患者使用他汀类药物与 COPD 加重风险降低无关。