Department of Respiratory Medicine, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark.
Clinical Research Centre, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark.
Int J Chron Obstruct Pulmon Dis. 2021 Mar 5;16:579-589. doi: 10.2147/COPD.S296472. eCollection 2021.
Statins have, due to their anti-inflammatory properties, been suggested to potentially improve chronic obstructive pulmonary disease (COPD) outcomes. We aimed to investigate the effect of statins on time to first exacerbation and all-cause mortality in high-risk COPD outpatients.
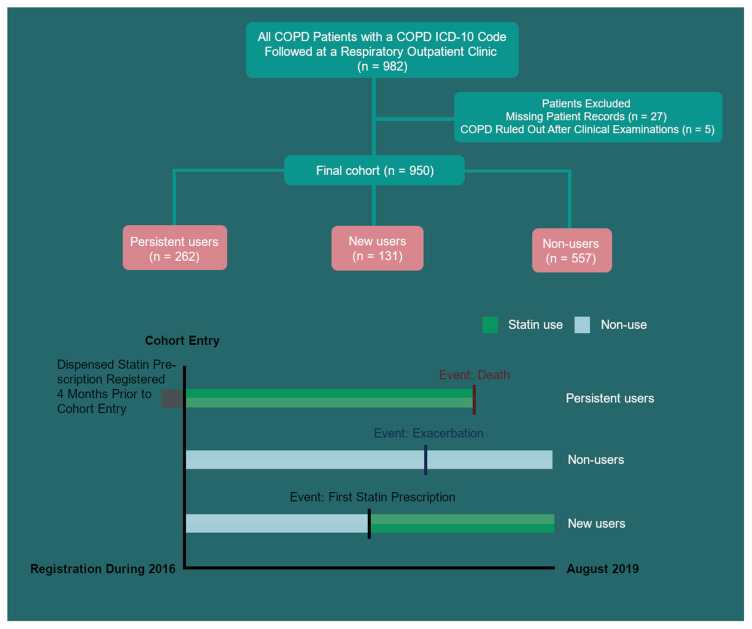
All outpatients with COPD seen at the Department of Respiratory Medicine, Copenhagen University Hospital Amager and Hvidovre, Denmark in 2016 were identified and followed for 3.5 years in this retrospective, registry-based cohort study of time to first acute exacerbation of COPD (AECOPD) or death. AECOPD was defined as a rescue course of oral corticosteroid and/or hospital admission. The association was estimated using time-varying crude and multivariable Cox proportional hazard regression.
The cohort comprised 950 COPD outpatients, mean (SD) age 71 (11) years, and FEV1 44% predicted (IQR 33%; 57%). The annual exacerbation rate was 0.88 (1.68) and 211 patients (22%) had a history of hospital admission for AECOPD in the 12 months prior to index date. Three hundred and ninety-three patients (41.4%) were defined as statin users, with 131 (33.3%) having filled the first prescription for statin after index date. Statin use was not associated with reduced risk of AECOPD. When stratifying for moderate and severe exacerbations in a sub-analysis in the same model, statin use did not have an increased HR for exacerbation of either severity (HR = 1.02 (95% CI 0.85to 1.24; p = 0.811) and HR = 1.07 (95% CI 0.89 to 1.29; p = 0.492) respectively). Statin use was not associated with all-cause mortality (HR 1.05 (95% CI, 0.75 to 1.47, p = 0.777)).
We did not find any association between statin use and risk of AECOPD or all-cause mortality. The result adds to the evidence that an aggressive approach with statin treatment upfront is not beneficial in COPD, unless prescribed according to current guidelines for cardiovascular diseases.
由于他汀类药物具有抗炎特性,因此有人提出他汀类药物可能改善慢性阻塞性肺疾病(COPD)的预后。我们旨在研究他汀类药物对高危 COPD 门诊患者首次加重时间和全因死亡率的影响。
在丹麦哥本哈根大学医院阿迈厄和维德霍夫呼吸医学系 2016 年就诊的所有 COPD 门诊患者均被确定为研究对象,并在这项 COPD 首次急性加重(AECOPD)或死亡时间的回顾性基于登记的队列研究中随访 3.5 年。AECOPD 定义为口服皮质类固醇和/或住院治疗的抢救疗程。使用时间变化的粗和多变量 Cox 比例风险回归估计关联。
该队列包括 950 例 COPD 门诊患者,平均(SD)年龄 71(11)岁,FEV1 占预计值的 44%(IQR 33%;57%)。每年加重率为 0.88(1.68),211 例患者(22%)在指数日期前 12 个月内有因 AECOPD 住院治疗的病史。393 例患者(41.4%)被定义为他汀类药物使用者,其中 131 例(33.3%)在指数日期后首次开具了他汀类药物处方。他汀类药物的使用与 AECOPD 风险降低无关。在同一模型的亚分析中对中重度加重进行分层时,他汀类药物的使用对两种严重程度的加重均无增加的 HR(HR = 1.02(95%CI 0.85 至 1.24;p = 0.811)和 HR = 1.07(95%CI 0.89 至 1.29;p = 0.492))。他汀类药物的使用与全因死亡率无关(HR 1.05(95%CI,0.75 至 1.47,p = 0.777))。
我们没有发现他汀类药物的使用与 AECOPD 风险或全因死亡率之间存在任何关联。该结果增加了证据,即除非根据心血管疾病的现行指南规定进行处方,否则积极使用他汀类药物治疗不会使 COPD 受益。