START Madrid-FJD, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain.
Medical Oncology, Catalan Institute of Oncology, Girona, Spain.
J Immunother Cancer. 2021 Dec;9(12). doi: 10.1136/jitc-2021-003645.
Treatment outcomes remain poor in recurrent platinum-resistant ovarian cancer. Enadenotucirev, a tumor-selective and blood stable adenoviral vector, has demonstrated a manageable safety profile in phase 1 studies in epithelial solid tumors.
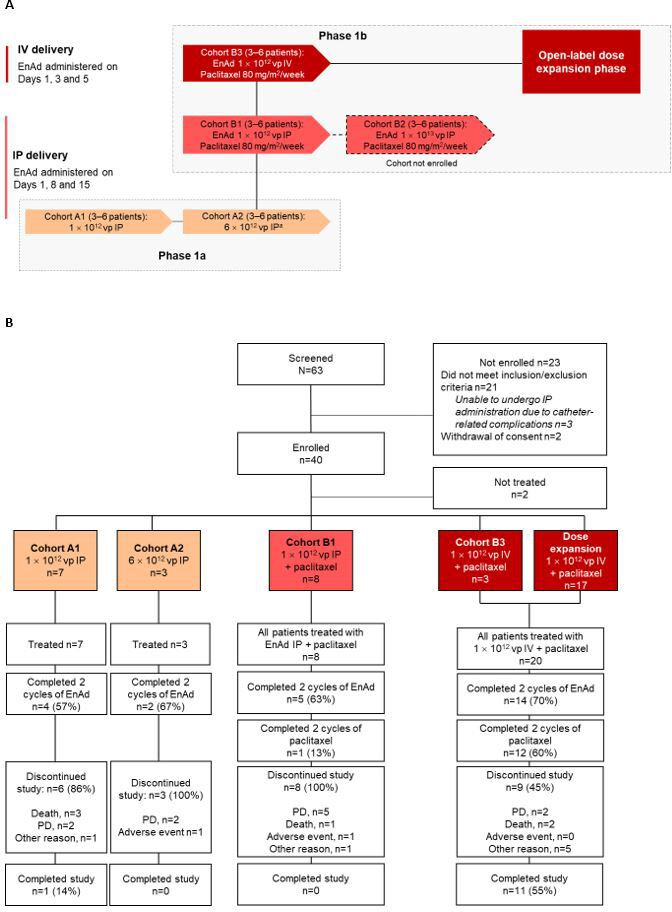
We conducted a multicenter, open-label, phase 1 dose-escalation and dose-expansion study (OCTAVE) to assess enadenotucirev plus paclitaxel in patients with platinum-resistant epithelial ovarian cancer. During phase 1a, the maximum tolerated dose of intraperitoneally administered enadenotucirev monotherapy (three doses; days 1, 8 and 15) was assessed using a 3+3 dose-escalation model. Phase 1b included a dose-escalation and an intravenous dosing dose-expansion phase assessing enadenotucirev plus paclitaxel. For phase 1a/b, the primary objective was to determine the maximum tolerated dose of enadenotucirev (with paclitaxel in phase 1b). In the dose-expansion phase, the primary endpoint was progression-free survival (PFS). Additional endpoints included response rate and T-cell infiltration.
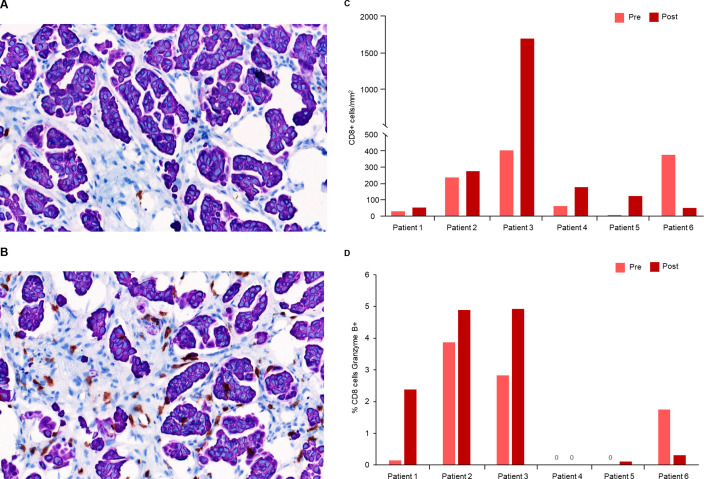
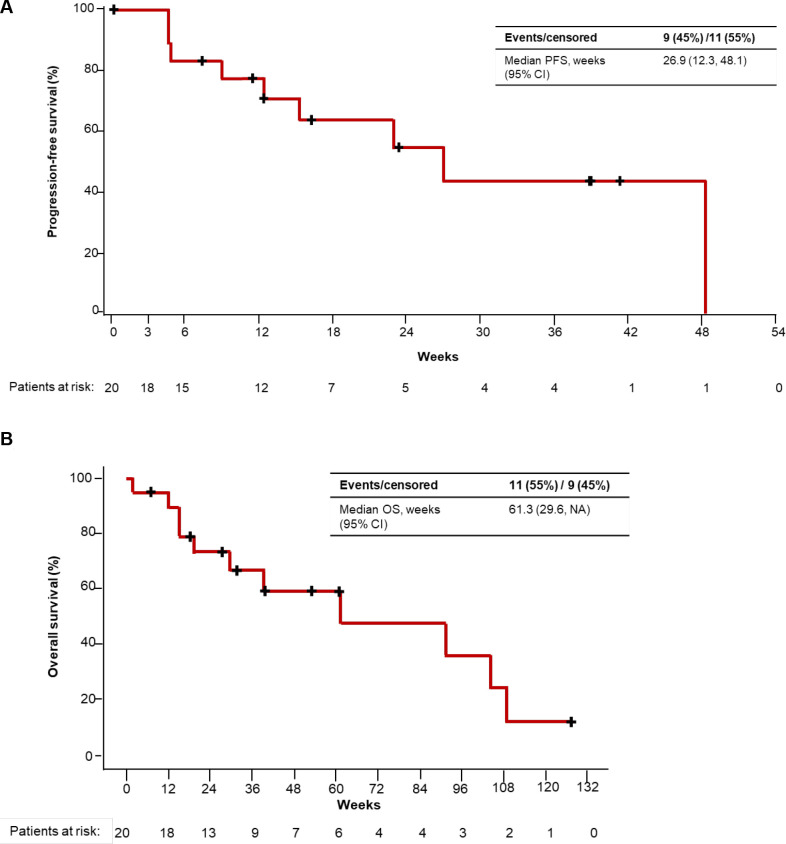
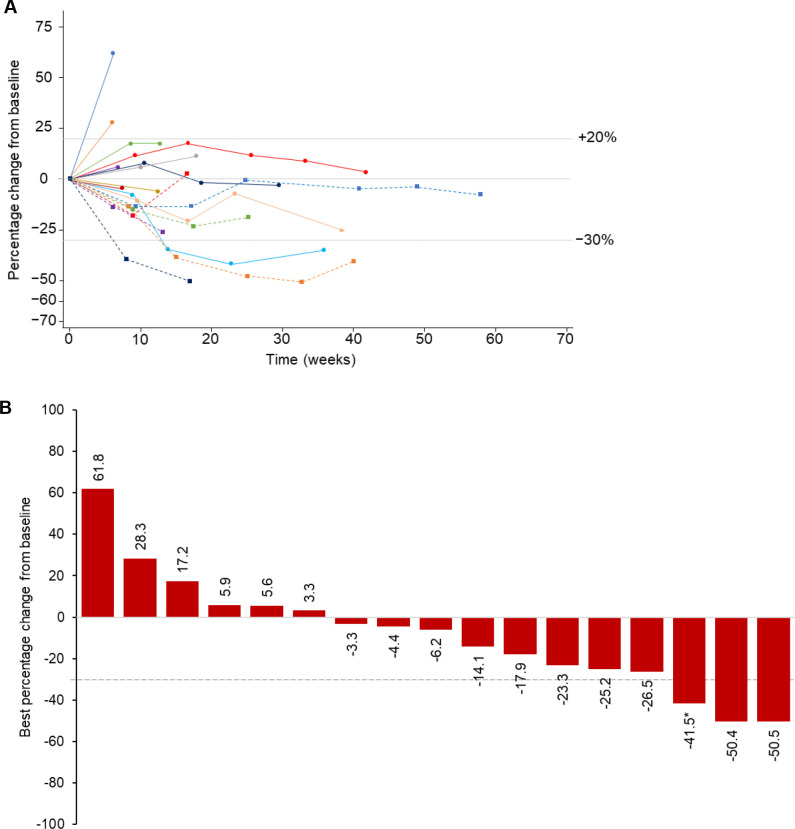
Overall, 38 heavily pretreated patients were enrolled and treated. No dose-limiting toxicities were observed at any doses. However, frequent catheter complications led to the discontinuation of intraperitoneal dosing during phase 1b. Intravenous enadenotucirev (1×10 viral particles; days 1, 3 and 5 every 28-days for two cycles) plus paclitaxel (80 mg/m; days 9, 16 and 23 of each cycle) was thus selected for dose-expansion. Overall, 24/38 (63%) patients experienced at least 1 Grade ≥3 treatment-emergent adverse event (TEAE); most frequently neutropenia (21%). Six patients discontinued treatment due to TEAEs, including one patient due to a grade 2 treatment-emergent serious AE of catheter site infection (intraperitoneal enadenotucirev monotherapy). Among the 20 patients who received intravenous enadenotucirev plus paclitaxel, 4-month PFS rate was 64% (median 6.2 months), objective response rate was 10%, 35% of patients achieved stable disease and 65% of patients had a reduction in target lesion burden at ≥1 time point. Five out of six patients with matched pre-treatment and post-treatment biopsies treated with intravenous enadenotucirev plus paclitaxel had increased (mean 3.1-fold) infiltration of CD8 +T cells in post-treatment biopsies.
Intravenously dosed enadenotucirev plus paclitaxel demonstrated manageable tolerability, an encouraging median PFS and increased tumor immune-cell infiltration in platinum-resistant ovarian cancer.
NCT02028117.
复发性铂耐药卵巢癌的治疗效果仍然很差。Enadenotucirev 是一种肿瘤选择性和血液稳定的腺病毒载体,在上皮实体肿瘤的 1 期研究中表现出可管理的安全性。
我们进行了一项多中心、开放标签、1 期剂量递增和扩展研究(OCTAVE),以评估 Enadenotucirev 联合紫杉醇治疗铂耐药上皮性卵巢癌患者。在 1a 期,采用 3+3 剂量递增模型评估腹腔内给予 Enadenotucirev 单药治疗(3 剂;第 1、8 和 15 天)的最大耐受剂量。1b 期包括剂量递增和静脉给药剂量扩展期,评估 Enadenotucirev 联合紫杉醇。对于 1a/b 期,主要目的是确定 Enadenotucirev 的最大耐受剂量(在 1b 期用紫杉醇)。在剂量扩展阶段,主要终点是无进展生存期(PFS)。其他终点包括反应率和 T 细胞浸润。
共有 38 名接受过多重预处理的患者入组并接受治疗。在任何剂量下均未观察到剂量限制毒性。然而,频繁的导管并发症导致在 1b 期停止了腹腔内给药。因此,选择静脉注射 Enadenotucirev(1×10 病毒颗粒;每 28 天静脉注射两次,第 1、3 和 5 天,共两个周期)联合紫杉醇(80mg/m;每个周期的第 9、16 和 23 天)进行剂量扩展。总体而言,38 例患者中有 24 例(63%)至少发生 1 例≥3 级治疗后出现的不良事件(TEAE);最常见的是中性粒细胞减少症(21%)。6 名患者因 TEAEs 而停止治疗,包括 1 名因腹腔内 Enadenotucirev 单药治疗时出现 2 级治疗后严重的与治疗相关的感染性导管部位不良事件而停止治疗。在接受静脉注射 Enadenotucirev 联合紫杉醇的 20 名患者中,4 个月的 PFS 率为 64%(中位 PFS 6.2 个月),客观缓解率为 10%,35%的患者疾病稳定,65%的患者在至少 1 个时间点时肿瘤靶病灶负荷减少。在接受静脉注射 Enadenotucirev 联合紫杉醇治疗的 6 名具有匹配的治疗前和治疗后活检的患者中,有 5 名患者的 CD8+T 细胞浸润增加(平均增加 3.1 倍)。
静脉注射 Enadenotucirev 联合紫杉醇具有可管理的耐受性,铂耐药卵巢癌患者的中位 PFS 令人鼓舞,并且肿瘤免疫细胞浸润增加。
NCT02028117。