Vestergaard Lone Due, Lauridsen Kasper Glerup, Krarup Niels Henrik Vinther, Kristensen Jane Uhrenholt, Andersen Lone Kaerslund, Løfgren Bo
Department of Cardiology, Lillebaelt Hospital, Vejle, Denmark.
Department of Internal Medicine, Randers Regional Hospital, Randers, Denmark.
Open Access Emerg Med. 2021 Dec 16;13:553-560. doi: 10.2147/OAEM.S341479. eCollection 2021.
To improve cardiac arrest survival, international resuscitation guidelines emphasize measuring the quality of cardiopulmonary resuscitation (CPR). We aimed to investigate CPR quality during in-hospital cardiac arrest (IHCA) and study long-term survival outcomes.
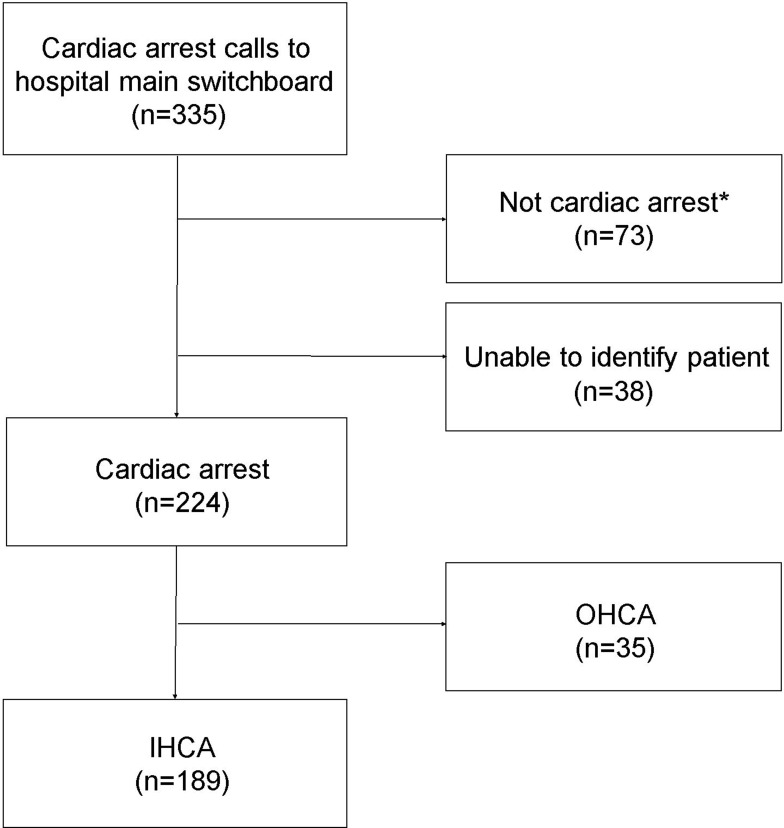
This was a cohort study of IHCA from December 2011 until November 2014. Data were collected from the hospital switch board, patient records, and from defibrillators. Impedance data from defibrillators were analyzed manually at the level of single compressions. Long-term survival at 1-, 3-, and 5 years is reported.
The study included 189 IHCAs; median (interquartile range (IQR)) time to first rhythm analysis was 116 (70-201) seconds and median (IQR) time to first defibrillation was 133 (82-264) seconds. Median (IQR) chest compression rate was 126 (119-131) per minute and chest compression fraction (CCF) was 78% (69-86). Thirty-day survival was 25%, while 1-year-, 3-year-, and 5-year survival were 21%, 14%, and 13%, respectively. There was no significant association between any survival outcomes and CCF, whereas chest compression rate was associated with survival to 30 days and 3 years. Overall, 5-year survival was associated with younger age (median 68 vs 74 years, =0.003), less comorbidity (Charlson comorbidity index median 3 vs 5, <0.001), and witnessed cardiac arrest (96% vs 77%, =0.03).
We established a systematic collection of IHCA CPR quality data to measure and improve CPR quality and long-term survival outcomes. Median time to first rhythm check/defibrillation was <3 minutes, but median chest compression rate was too fast and median CCF slightly below 80%. More than half of 30-day survivors were still alive at 5 years.
为提高心脏骤停的生存率,国际复苏指南强调要对心肺复苏(CPR)的质量进行评估。我们旨在调查院内心脏骤停(IHCA)期间的心肺复苏质量,并研究长期生存结局。
这是一项针对2011年12月至2014年11月期间院内心脏骤停患者的队列研究。数据收集自医院总机、患者病历以及除颤器。除颤器的阻抗数据在单次按压水平上进行人工分析。报告了1年、3年和5年的长期生存率。
该研究纳入了189例院内心脏骤停患者;首次心律分析的中位(四分位间距(IQR))时间为116(70 - 201)秒,首次除颤的中位(IQR)时间为133(82 - 264)秒。胸部按压的中位(IQR)频率为每分钟126次(119 - 131次),胸部按压分数(CCF)为78%(69 - 86)。30天生存率为25%,而1年、3年和5年生存率分别为21%、14%和13%。任何生存结局与胸部按压分数之间均无显著关联,而胸部按压频率与30天和3年生存率相关。总体而言,5年生存率与较年轻的年龄(中位年龄68岁对74岁,P = 0.003)、较少的合并症(Charlson合并症指数中位值3对5,P < 0.001)以及目击心脏骤停(96%对77%,P = 0.03)相关。
我们建立了院内心脏骤停心肺复苏质量数据的系统收集方法,以评估和改善心肺复苏质量及长期生存结局。首次心律检查/除颤的中位时间<3分钟,但胸部按压的中位频率过快,胸部按压分数的中位值略低于80%。超过一半的30天幸存者在5年后仍然存活。