Alese Olatunji B, Zhou Wei, Jiang Renjian, Zakka Katerina, Huang Zhonglu, Okoli Chimuanya, Shaib Walid L, Akce Mehmet, Diab Maria, Wu Christina, El-Rayes Bassel F
Department of Hematology and Medical Oncology, Winship Cancer Institute, Emory University, Atlanta, GA, United States.
Winship Data and Technology Applications Shared Resource, Emory University, Atlanta, GA, United States.
Front Oncol. 2021 Dec 9;11:728076. doi: 10.3389/fonc.2021.728076. eCollection 2021.
Pathologic staging is crucial in colorectal cancer (CRC). Unlike the majority of solid tumors, the current staging model does not use tumor size as a criterion. We evaluated the predictive and prognostic impact of primary tumor size on all stages of CRC.
Using the National Cancer Database (NCDB), we conducted an analysis of CRC patients diagnosed between 2010 and 2015 who underwent resection of their primary cancer. Univariate and multivariate analyses were used to identify predictive and prognostic factors, Kaplan-Meier analysis and Cox proportional hazards models for association between tumor size and survival.
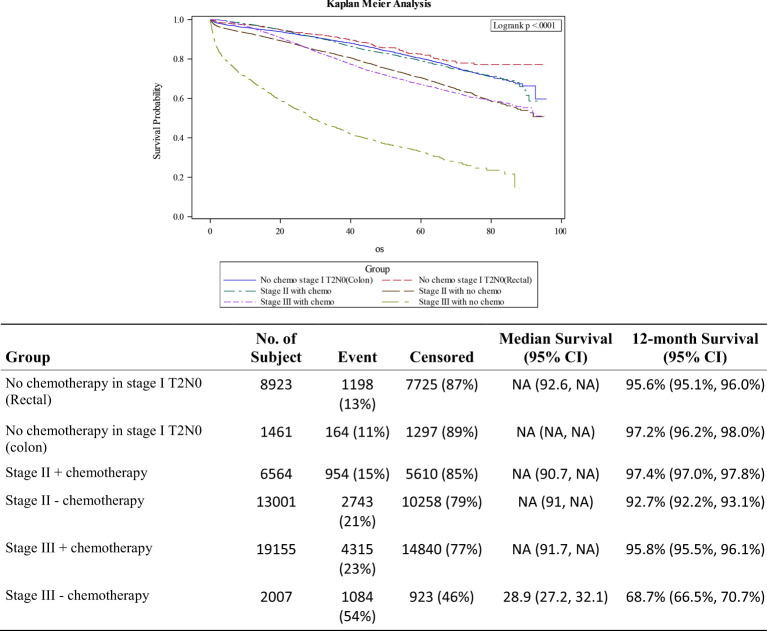
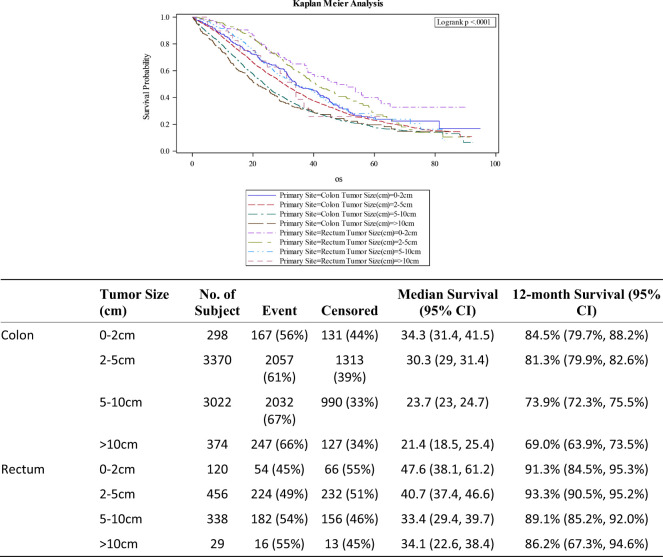
About 61,000 patients met the inclusion criteria. Median age was 63 years and majority of the tumors were colon primary (82.7%). AJCC stage distribution was: I - 20.1%; II - 32.1%; III - 34.7% and IV - 13.1%. The prognostic impact of tumor size was strongly associated with survival in stage III disease. Compared to patients with tumors <2cm; those with 2-5cm (HR 1.33; 1.19-1.49; p<0.001), 5-10cm (HR 1.51 (1.34-1.70; p<0.001) and >10cm (HR 1.95 (1.65-2.31; p<0.001) had worse survival independent of other variables. Stage II treated without adjuvant chemotherapy had comparable survival outcomes (HR 1.09; 0.97-1.523; p=0.148) with stage III patients who did, while Stage II patients who received adjuvant chemotherapy did much better than both groups (HR 0.76; 0.67-0.86; p<0.001). Stage III patients who did not receive adjuvant chemotherapy had the worst outcomes among the non-metastatic disease subgroups (HR 2.66; 2.48-2.86; p<0.001). Larger tumors were associated with advanced stage, MSI high, non-rectal primary and positive resection margins.
Further studies are needed to clarify the role of tumor size in prognostic staging models, and how to incorporate it into therapy decisions.
病理分期在结直肠癌(CRC)中至关重要。与大多数实体瘤不同,当前的分期模型未将肿瘤大小作为一项标准。我们评估了原发性肿瘤大小对CRC各阶段的预测和预后影响。
利用国家癌症数据库(NCDB),我们对2010年至2015年间诊断为CRC且接受原发性癌症切除术的患者进行了分析。采用单因素和多因素分析来确定预测和预后因素,使用Kaplan-Meier分析和Cox比例风险模型来研究肿瘤大小与生存之间的关联。
约61000名患者符合纳入标准。中位年龄为63岁,大多数肿瘤为结肠原发性(82.7%)。美国癌症联合委员会(AJCC)分期分布为:I期 - 20.1%;II期 - 32.1%;III期 - 34.7%;IV期 - 13.1%。肿瘤大小的预后影响与III期疾病的生存密切相关。与肿瘤<2cm的患者相比,肿瘤大小为2 - 5cm(风险比[HR] 1.33;95%置信区间[CI] 1.19 - 1.49;p<0.001)、5 - 10cm(HR 1.51 [1.34 - 1.70;p<0.001])和>10cm(HR 1.95 [1.65 - 2.31;p<0.001])的患者在不考虑其他变量的情况下生存情况更差。未接受辅助化疗的II期患者与接受辅助化疗的III期患者生存结果相当(HR 1.09;0.97 - 1.523;p = 0.148),而接受辅助化疗的II期患者比这两组患者的生存情况都要好得多(HR 0.76;0.67 - 0.86;p<0.001)。在非转移性疾病亚组中,未接受辅助化疗的III期患者预后最差(HR 2.66;2.48 - 2.86;p<0.001)。较大的肿瘤与晚期、微卫星高度不稳定(MSI高)、非直肠原发性和手术切缘阳性相关。
需要进一步研究以阐明肿瘤大小在预后分期模型中的作用,以及如何将其纳入治疗决策。