School of Public and Community Health Sciences, University of Montana, Missoula, MT, United States; Center for Population Health Research, University of Montana, Missoula, MT, United States.
School of Public and Community Health Sciences, University of Montana, Missoula, MT, United States; Center for Population Health Research, University of Montana, Missoula, MT, United States.
Vaccine. 2022 Jan 31;40(5):765-773. doi: 10.1016/j.vaccine.2021.12.037. Epub 2021 Dec 24.
Typically, early childhood vaccination coverage in the U.S. is measured as the proportion of children by age 24 months who completed recommended vaccine series. However, these measures do not reflect whether vaccine doses were received at the ages recommended by the U.S. Advisory Committee on Immunization Practices, or whether children received vaccines concomitantly, per the ACIP recommended schedule. This study's objective was to quantify vaccine timeliness and prevalence of specific patterns of undervaccination in U.S. children ages 0-19 months.
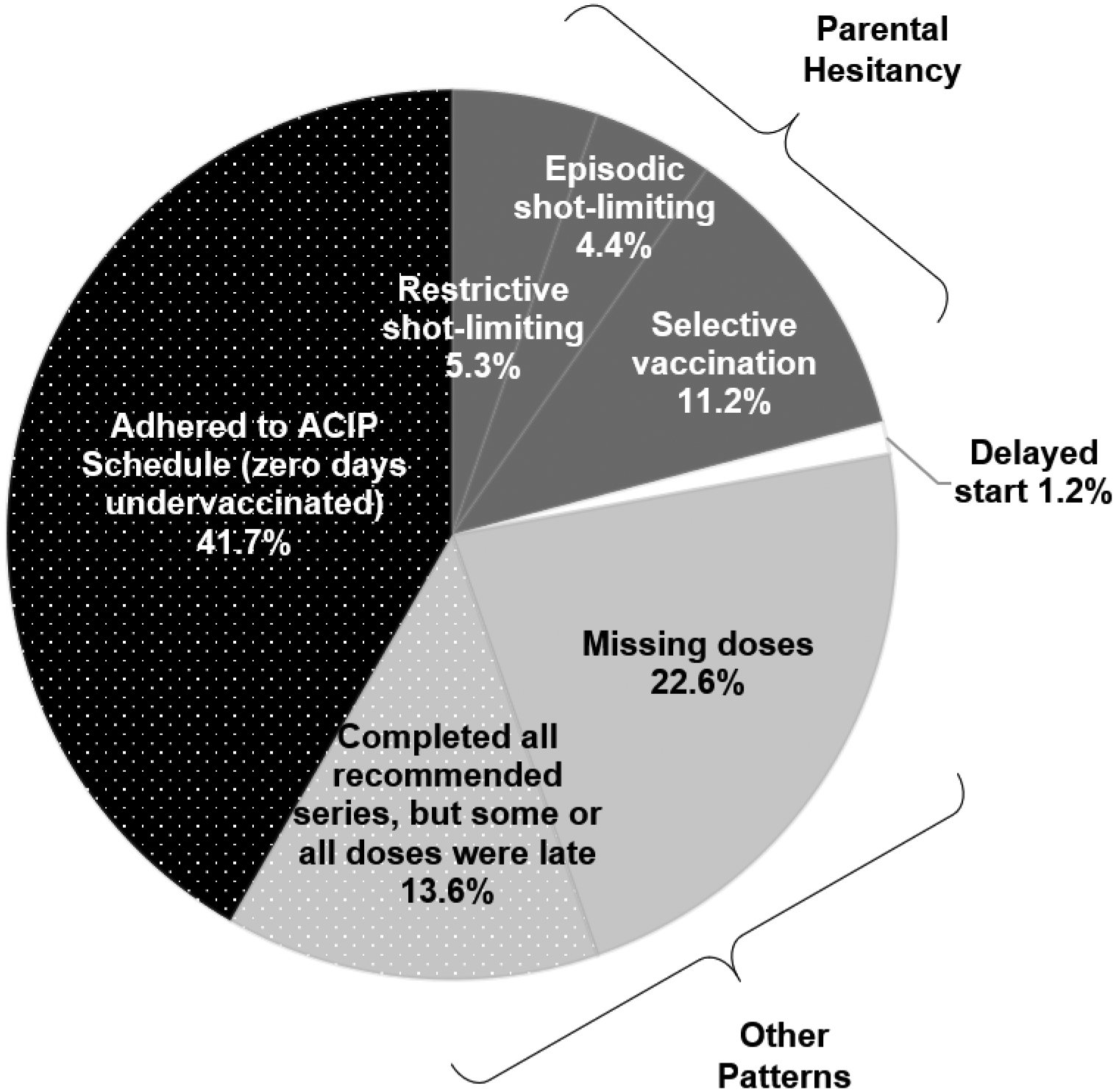
Using 2017 National Immunization Survey-Child data, we calculated days undervaccinated for the combined 7-vaccine series and distinguished undervaccination patterns indicative of parental vaccine hesitancy, such as spreading out vaccines across visits ("shot-limiting") or starting some but not all recommended vaccine series ("selective vaccination"), from other non-hesitancy patterns, such as missing final vaccine doses or receiving all doses, with some or all late. We measured associations between demographic, socioeconomic and other characteristics with undervaccination patterns using multivariable log-linked binomial regression. Analyses accounted for the complex survey design.
Among n = 15,333 U.S. children, only 41.2% received all recommended vaccine doses on-time by age 19 months. Approximately 20.9% of children had an undervaccination pattern suggestive of parental vaccine hesitancy, and 36.2% had other undervaccination non-hesitancy patterns. Uninsured children and those with lower levels of maternal education were more likely to exhibit undervaccination patterns suggestive of parental hesitancy. Lower levels of maternal education were also associated with other non-hesitancy undervaccination patterns.
More than half of children in the U.S. are undervaccinated at some point by 19 months of age. Ongoing assessment of vaccine timeliness and immunization schedule adherence could facilitate timely and targeted public health interventions in populations with high levels of undervaccination.
通常,美国的儿童早期疫苗接种覆盖率是通过测量 24 月龄以下儿童完成推荐疫苗系列的比例来衡量的。然而,这些措施并不能反映疫苗剂量是否是按照美国免疫实践咨询委员会推荐的年龄接种的,也不能反映儿童是否按照 ACIP 推荐的时间表同时接种疫苗。本研究的目的是量化美国 0-19 个月儿童疫苗接种的及时性和特定的疫苗接种不足模式的流行程度。
使用 2017 年国家免疫调查-儿童数据,我们计算了联合 7 价疫苗系列的疫苗接种不足天数,并区分了表明父母疫苗犹豫的疫苗接种不足模式,例如在就诊期间分散疫苗接种(“限制接种”)或开始接种部分但不是所有推荐疫苗系列(“选择性接种”),以及其他非犹豫模式,例如错过最后一剂疫苗或接种所有剂量,但有些或所有剂量延迟。我们使用多变量对数链接二项式回归来衡量人口统计学、社会经济和其他特征与疫苗接种不足模式之间的关联。分析考虑了复杂的调查设计。
在 15333 名美国儿童中,只有 41.2%的儿童在 19 个月龄时按时接受了所有推荐的疫苗剂量。约 20.9%的儿童存在父母疫苗犹豫的疫苗接种不足模式,36.2%的儿童存在其他非犹豫的疫苗接种不足模式。未参保儿童和受教育程度较低的儿童更有可能表现出父母犹豫的疫苗接种不足模式。较低的母亲教育水平也与其他非犹豫的疫苗接种不足模式相关。
在美国,超过一半的儿童在 19 个月龄时至少有一次疫苗接种不足。持续评估疫苗接种的及时性和免疫接种计划的遵守情况,可以促进在疫苗接种不足率较高的人群中及时采取有针对性的公共卫生干预措施。