Lee Haekyung, Kwon Soon Hyo, Jeon Jin Seok, Noh Hyunjin, Han Dong Cheol, Kim Hyoungnae
Division of Nephrology, Department of Internal Medicine, Soonchunhyang University Seoul Hospital, Seoul, Republic of Korea.
Hyonam Kidney Laboratory, Soonchunhyang University Seoul Hospital, Seoul, Republic of Korea.
Kidney Res Clin Pract. 2022 Jan;41(1):31-42. doi: 10.23876/j.krcp.21.099. Epub 2021 Nov 17.
Although hypertension is a well-known risk factor for chronic kidney disease (CKD), the blood pressure (BP) at which antihypertensive interventions should be initiated remains to be determined. Therefore, we investigated the association between BP and CKD in treatment-naïve individuals.
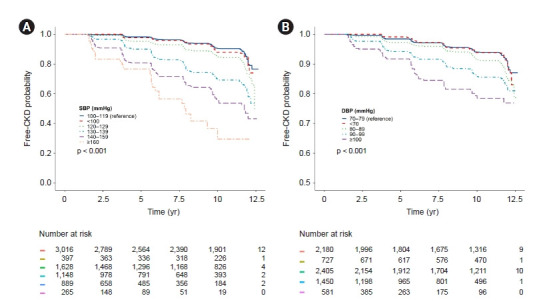
This prospective cohort study considered 7,343 individuals in the Korean Genome and Epidemiology Study who were not taking antihypertensive medications. Subjects were categorized into six groups according to their systolic BP (SBP) and five groups according to their diastolic BP (DBP). The primary outcome was incident CKD, which was defined as an estimated glomerular filtration rate of <60 mL/min/1.73 m2 or the development of proteinuria. The secondary outcome was incident cardiovascular disease (CVD).
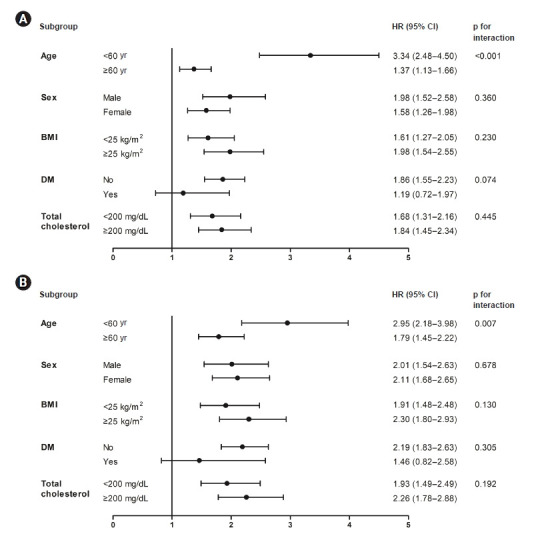
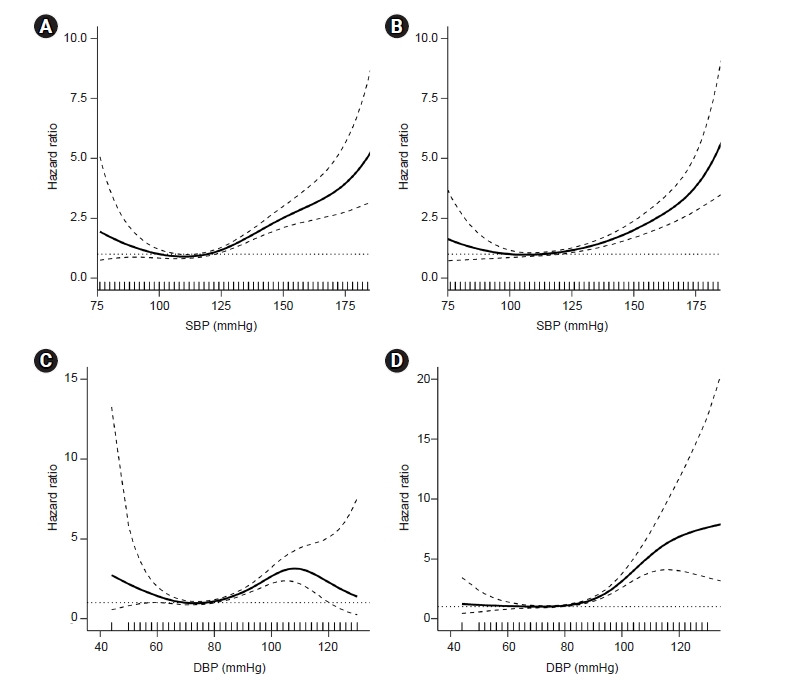
In the time-varying Cox models, the hazard ratios (95% confidence interval [CI]) for CKD were 1.39 (1.10-1.77) with SBP 130-139 mmHg, 1.79 (1.40-2.28) with SBP 140-159 mmHg, and 3.22 (2.35-4.40) with SBP ≥ 160 mmHg, compared with SBP 100-119 mmHg. In addition, the hazard ratios (95% CI) for CKD were 1.88 (1.48-2.37) with DBP 90-99 mmHg and 4.30 (3.20-5.76) with DBP ≥ 100 mmHg, compared with DBP 70-79 mmHg. A significantly increased CVD risk was also observed in subjects with SBP ≥ 130 mmHg or DBP ≥ 90 mmHg.
Our findings indicate that SBP ≥ 130 mmHg and DBP ≥ 90 mmHg are associated with an increased risk of CKD. Therefore, BP-lowering strategies should be considered starting at those thresholds to prevent CKD development.
尽管高血压是慢性肾脏病(CKD)的一个众所周知的危险因素,但启动降压干预的血压水平仍有待确定。因此,我们调查了未接受治疗的个体中血压与CKD之间的关联。
这项前瞻性队列研究纳入了韩国基因组与流行病学研究中的7343名未服用降压药物的个体。根据收缩压(SBP)将受试者分为六组,根据舒张压(DBP)分为五组。主要结局是新发CKD,定义为估计肾小球滤过率<60 mL/(min·1.73 m²)或出现蛋白尿。次要结局是新发心血管疾病(CVD)。
在时变Cox模型中,与SBP 100 - 119 mmHg相比,SBP 130 - 139 mmHg时CKD的风险比(95%置信区间[CI])为1.39(1.10 - 1.77),SBP 140 - 159 mmHg时为1.79(1.40 - 2.28),SBP≥160 mmHg时为3.22(2.35 - 4.40)。此外,与DBP 70 - 79 mmHg相比,DBP 90 - 99 mmHg时CKD的风险比(95%CI)为1.88(1.48 - 2.37),DBP≥100 mmHg时为4.30(3.20 - 5.76)。在SBP≥130 mmHg或DBP≥90 mmHg的受试者中也观察到CVD风险显著增加。
我们的研究结果表明,SBP≥130 mmHg和DBP≥90 mmHg与CKD风险增加相关。因此,应考虑从这些阈值开始采取降压策略以预防CKD的发生。