Department of Internal Medicine, Soonchunhyang University Seoul Hospital, Seoul, Republic of Korea.
Department of Medical Science, School of Medicine, Ewha Womans University, Seoul, Republic of Korea.
Sci Rep. 2020 Dec 9;10(1):21538. doi: 10.1038/s41598-020-78641-3.
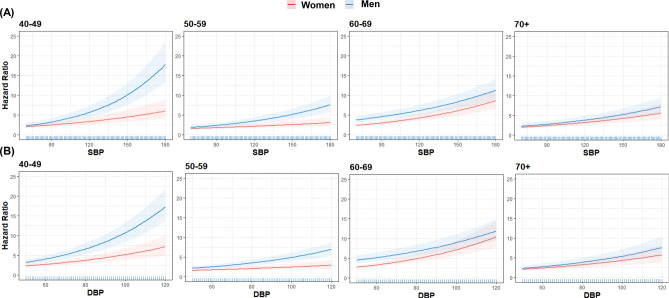
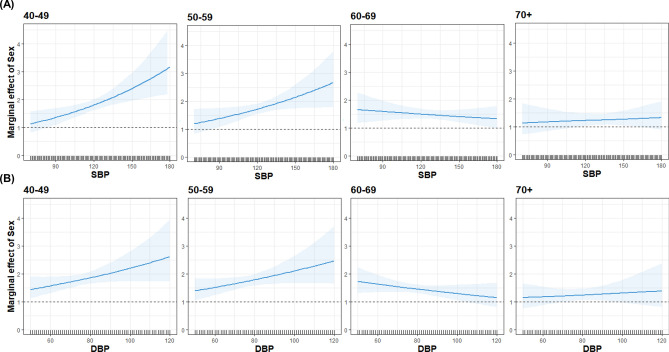
The time at which hypertension treatment should be initiated for different age groups and sexes remains controversial. We aimed to determine whether the association between blood pressure (BP) and major adverse cardiovascular events (MACE) varies with age and sex. This study enrolled 327,328 subjects who had not taken antihypertensive medication in the Korean National Health Service-National Health Screening Cohort between 2002 and 2003. Participants were categorized into four groups according to 2017 American College of Cardiology/American Heart Association hypertension guideline. Primary outcome was MACE characterized by cardiovascular mortality, myocardial infarction, unstable angina, and stroke. During a 10-year follow-up, a significant increase in MACE risk was observed from the stage 1 hypertension group (hazard ratio [HR], 1.23; 95% CI 1.15-1.32; P < 0.001) in time-varying Cox analysis. This relationship was persistent in subjects aged < 70 years, but increased MACE risk was observed only in the stage 2 hypertension group in ≥ 70 years (HR, 1.52; 95% CI 1.32-1.76, P < 0.001). When categorized as per sex, both men and women showed significant MACE risk from stage 1 hypertension. However, on comparing the sexes after stratifying by age, a significantly increased risk of MACE was shown from stage 1 hypertension in men aged < 50 years, but from stage 2 hypertension in men aged ≥ 50 years. Meanwhile, increased MACE risk was observed from stage 2 hypertension in women aged < 60 years, but from stage 1 hypertension in women aged ≥ 60 years. Thus, young male subjects had higher MACE risk than young female subjects, but this difference gradually decreased with age and there was no difference between sexes in subjects aged ≥ 70 years. Therefore, our results suggest that hypertension treatment initiation may need to be individualized depending on age and sex.
对于不同年龄组和性别的高血压治疗起始时间仍存在争议。我们旨在确定血压(BP)与主要不良心血管事件(MACE)之间的关联是否随年龄和性别而变化。这项研究纳入了 2002 年至 2003 年期间在韩国国家卫生服务-国家健康筛查队列中未服用抗高血压药物的 327328 名受试者。根据 2017 年美国心脏病学会/美国心脏协会高血压指南,参与者被分为四组。主要结局是由心血管死亡率、心肌梗死、不稳定型心绞痛和中风组成的 MACE。在 10 年的随访期间,在时变 Cox 分析中,从 1 期高血压组(危险比[HR],1.23;95%置信区间 1.15-1.32;P<0.001)观察到 MACE 风险显著增加。这种关系在年龄<70 岁的受试者中仍然存在,但在≥70 岁的受试者中仅在 2 期高血压组中观察到增加的 MACE 风险(HR,1.52;95%置信区间 1.32-1.76,P<0.001)。按性别分类时,男性和女性均从 1 期高血压中显示出显著的 MACE 风险。然而,在按年龄分层后比较性别时,在年龄<50 岁的男性中从 1 期高血压开始,在年龄≥50 岁的男性中从 2 期高血压开始,MACE 风险显著增加。同时,在年龄<60 岁的女性中,从 2 期高血压开始,MACE 风险增加,但在年龄≥60 岁的女性中,从 1 期高血压开始,MACE 风险增加。因此,年轻男性受试者的 MACE 风险高于年轻女性,但这种差异随年龄逐渐减小,在年龄≥70 岁的受试者中,性别之间没有差异。因此,我们的结果表明,高血压治疗的开始可能需要根据年龄和性别进行个体化。