Nessel Regine, Löffler Thorsten, Rinn Johannes, Lösel Philipp, Voss Samuel, Heuveline Vincent, Vollmer Matthias, Görich Johannes, Ludwig Yannique-Maximilian, Al-Hileh Luai, Kallinowski Friedrich
General, Visceral and Pediatric Surgery, Klinikum Am Gesundbrunnen, Heilbronn, Germany.
General and Visceral Surgery, Gesundheitszentrum Rhein-Neckar Hospital Eberbach, Eberbach, Germany.
Front Surg. 2021 Dec 15;8:764470. doi: 10.3389/fsurg.2021.764470. eCollection 2021.
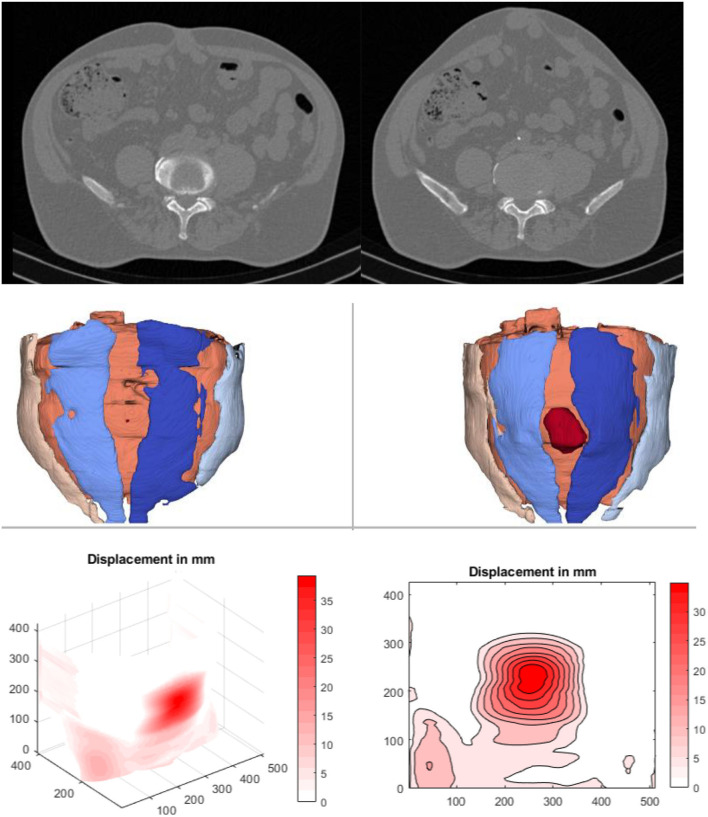
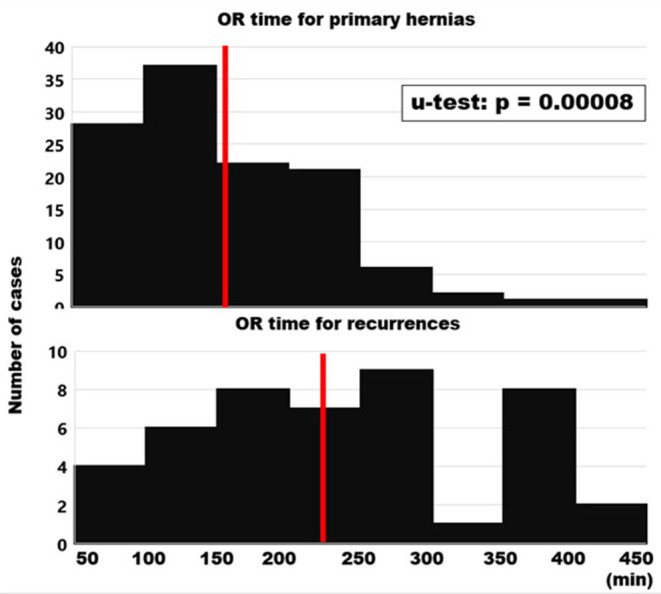
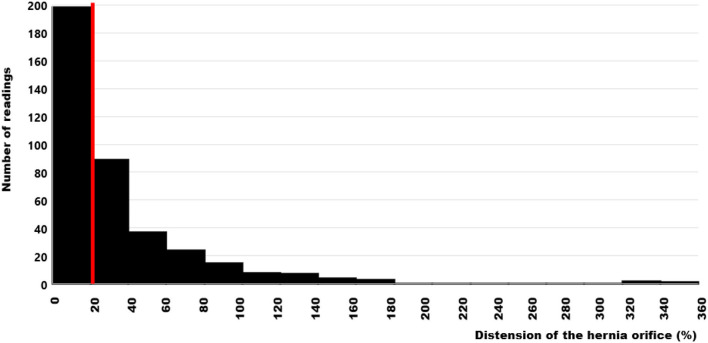
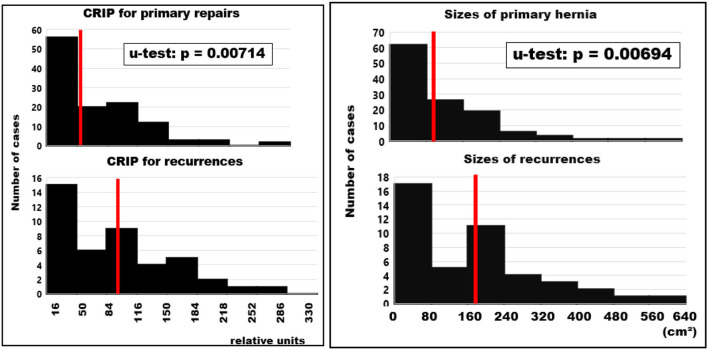
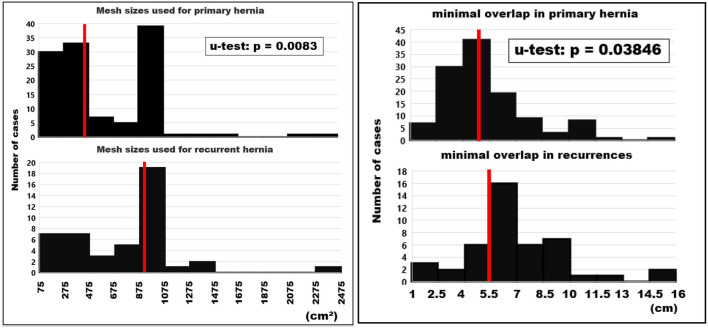
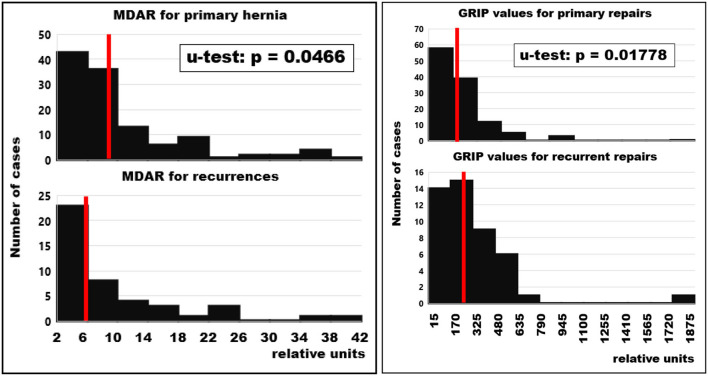
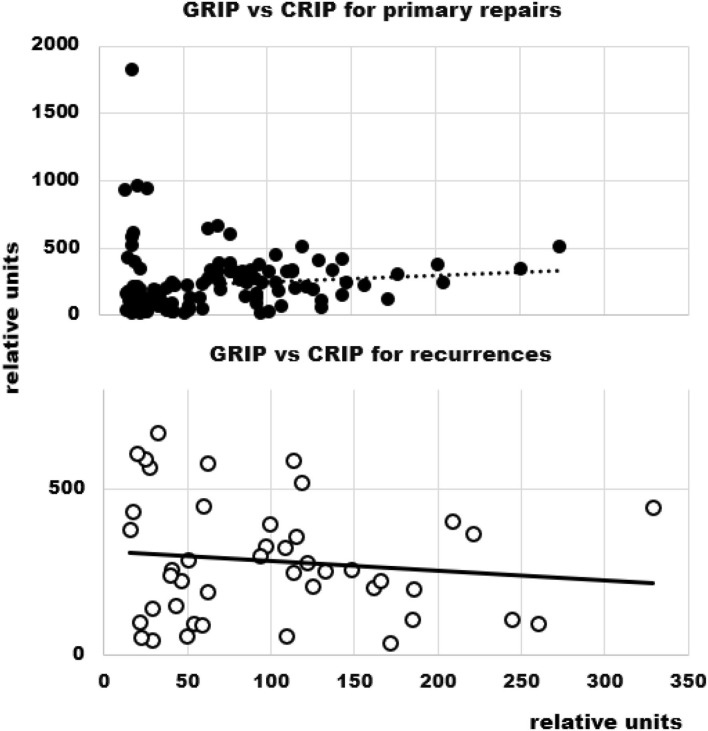
Mechanical principles successfully guide the construction of polymer material composites in engineering. Since the abdominal wall is a polymer composite augmented with a textile during incisional hernia repair we ask: can incisional hernia be repaired safely and durably based on biomechanical principles? Repair materials were assessed on a self-built bench test using pulse loads to elude influences on the reconstruction of the abdominal wall. Tissue elasticity was analyzed preoperatively as needed with computed tomography at rest and during Valsalva's maneuver. Preoperatively, the critical retention force of the reconstruction to pulse loads was calculated and a biomechanically durable repair was designed based on the needs of the individual patient. Intraoperatively, the design was adjusted as needed. Hernia meshes with high grip factors (Progrip, Dahlhausen Cicat) were used for the repairs. Mesh sizes, fixation elements and reconstructive details were oriented on the biomechanical design. All patients recieved single-shot antibiosis. Patients were discharged after full ambulation was achieved. A total of 163 patients (82 males and 81 females) were treated for incisional hernia in four hospitals by ten surgeons. Primary hernia was repaired in 119 patients. Recurrent hernia was operated on in 44 cases. Recurrent hernia was significantly larger (median 161 cm vs. 78 cm; u-test: = 0.00714). Re-do surgery took significantly longer (median 229 min vs. 150 min; < 0.00001) since recurrent disease required more often transversus abdominis release (70% vs. 47%). GRIP tended to be higher in recurrent repair ( = 0.01828). Complication rates (15%) and hospital stay were the same (6 vs. 6 days; = 0.28462). After 1 year, no recurrence was detected in either group. Pain levels were equally low in both primary and recurrent hernia repairs (median NAS = 0 in both groups at rest and under load, = 0.88866). Incisional hernia can safely and durably be repaired based on biomechanical principles both in primary and recurrent disease. The GRIP concept provides a base for the application of biomechanical principles in incisional hernia repair.
机械原理成功地指导了工程中聚合物材料复合材料的构建。由于腹壁是在切口疝修补术中用织物增强的聚合物复合材料,我们提出疑问:能否基于生物力学原理安全、持久地修复切口疝?使用脉冲载荷在自建的台架试验上评估修复材料,以避免对腹壁重建产生影响。根据需要,术前通过计算机断层扫描在静息状态和瓦尔萨尔瓦动作期间分析组织弹性。术前计算重建对脉冲载荷的临界保持力,并根据个体患者的需求设计生物力学上持久的修复方案。术中根据需要调整设计。使用具有高抓持因子的疝修补网片(Progrip、Dahlhausen Cicat)进行修复。网片尺寸、固定元件和重建细节均基于生物力学设计。所有患者均接受单次抗生素治疗。患者在能够完全行走后出院。四家医院的十名外科医生共治疗了163例切口疝患者(82例男性和81例女性)。119例患者修复了原发性疝。44例患者接受了复发性疝手术。复发性疝明显更大(中位数161平方厘米对78平方厘米;u检验:=0.00714)。再次手术时间明显更长(中位数229分钟对150分钟;<0.00001),因为复发性疾病更常需要腹横肌松解(70%对47%)。复发性修复中的抓持力往往更高(=0.01828)。并发症发生率(15%)和住院时间相同(6天对6天;=0.28462)。1年后,两组均未检测到复发。原发性和复发性疝修补术后的疼痛程度同样较低(两组静息和负重时NAS中位数均为0,=0.88866)。基于生物力学原理,无论是原发性还是复发性疾病,切口疝都可以安全、持久地修复。抓持力概念为生物力学原理在切口疝修补术中的应用提供了基础。