Kallinowski Friedrich, Harder F, Gutjahr D, Raschidi R, Silva T G, Vollmer M, Nessel Regine
Klinik für Allgemein-, Visceral- und Transplantationschirurgie, Chirurgische Universitätsklinik Heidelberg, Heidelberg, Germany.
Institut für Biomechanik, Technische Universität Hamburg-Harburg, Hamburg, Germany.
Front Surg. 2018 Jan 19;4:78. doi: 10.3389/fsurg.2017.00078. eCollection 2017.
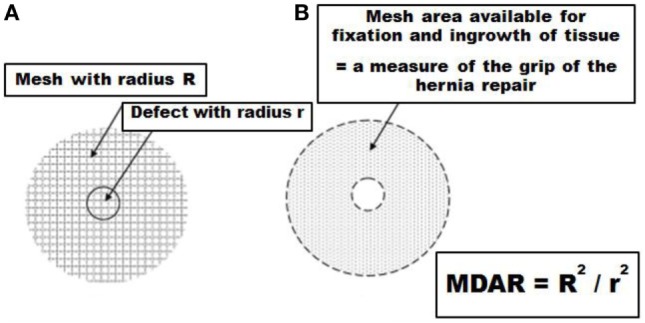
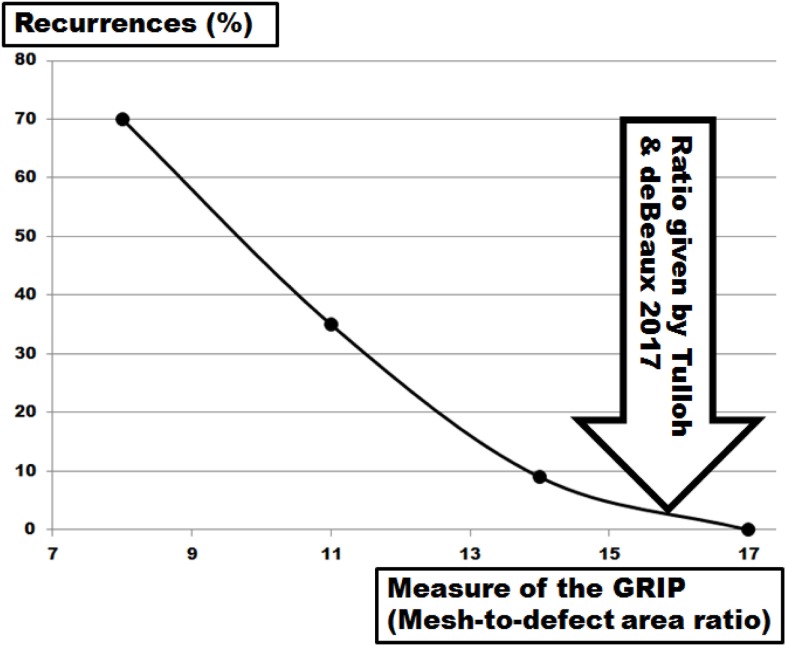
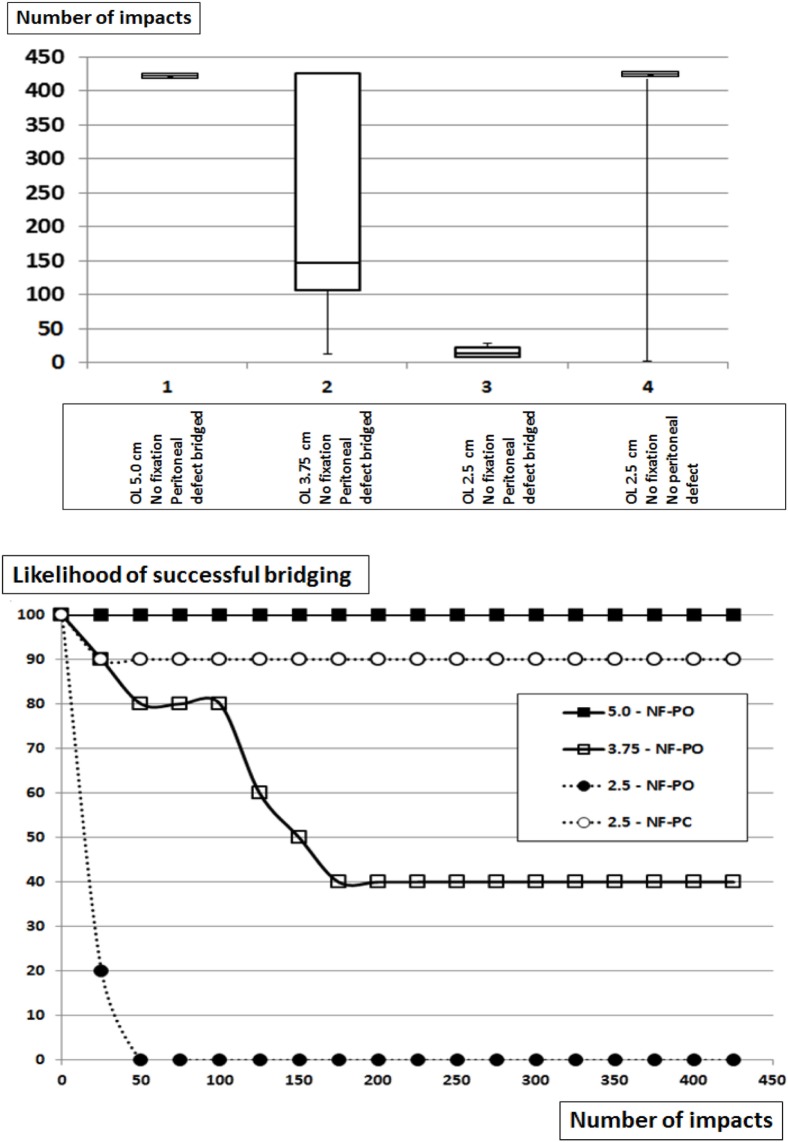
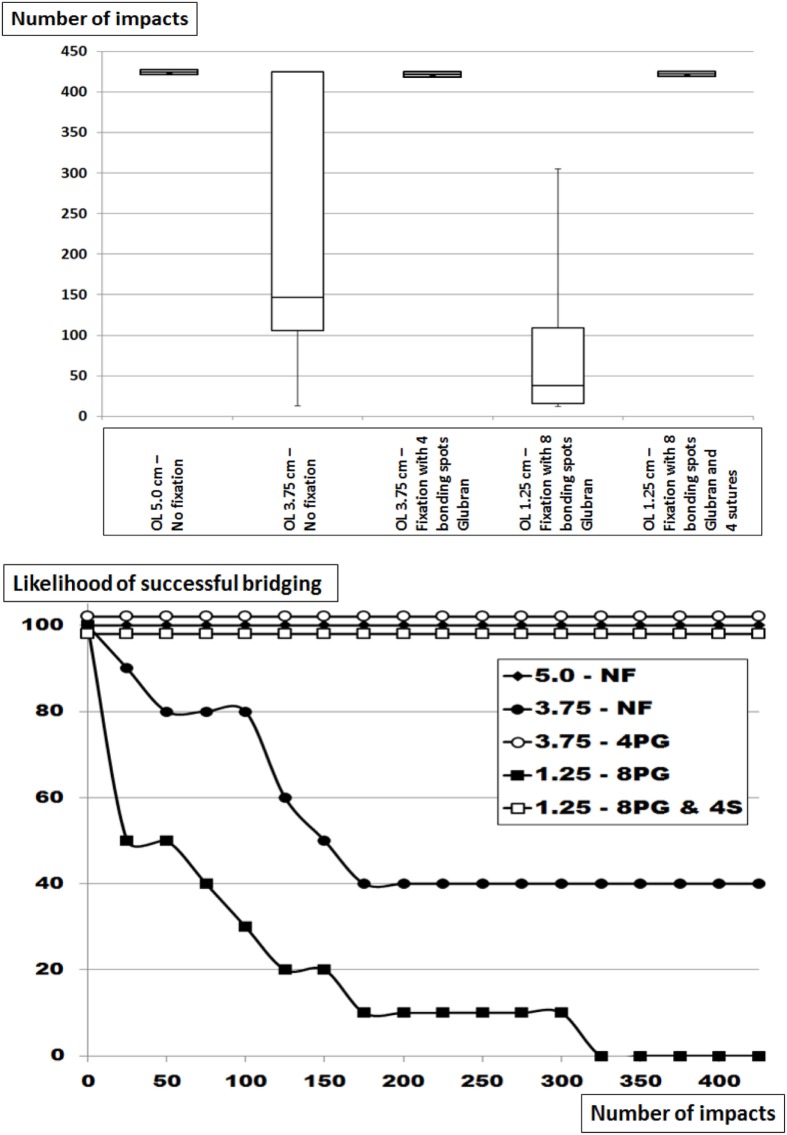
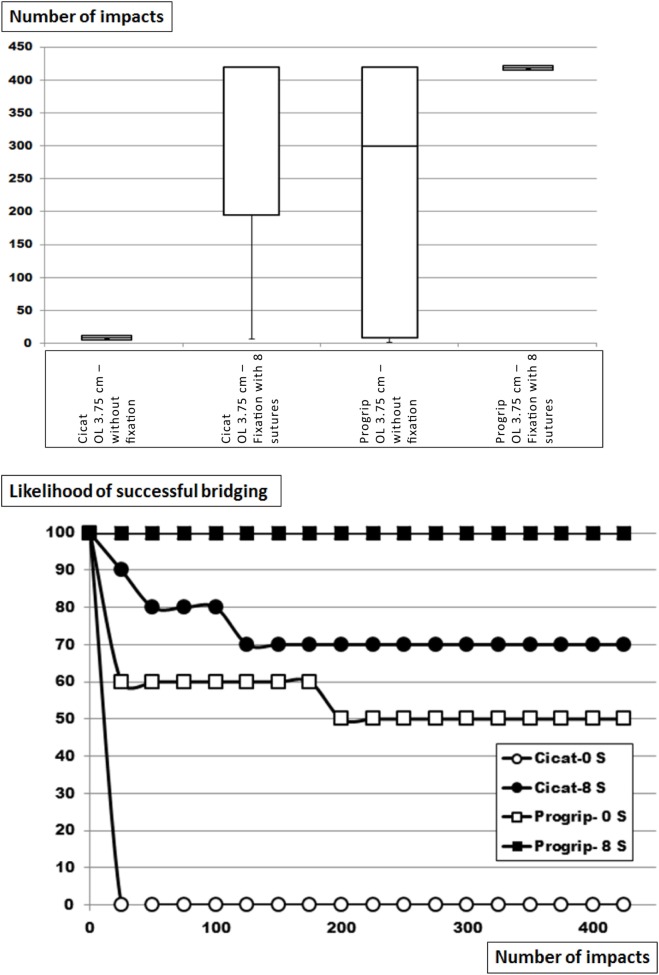
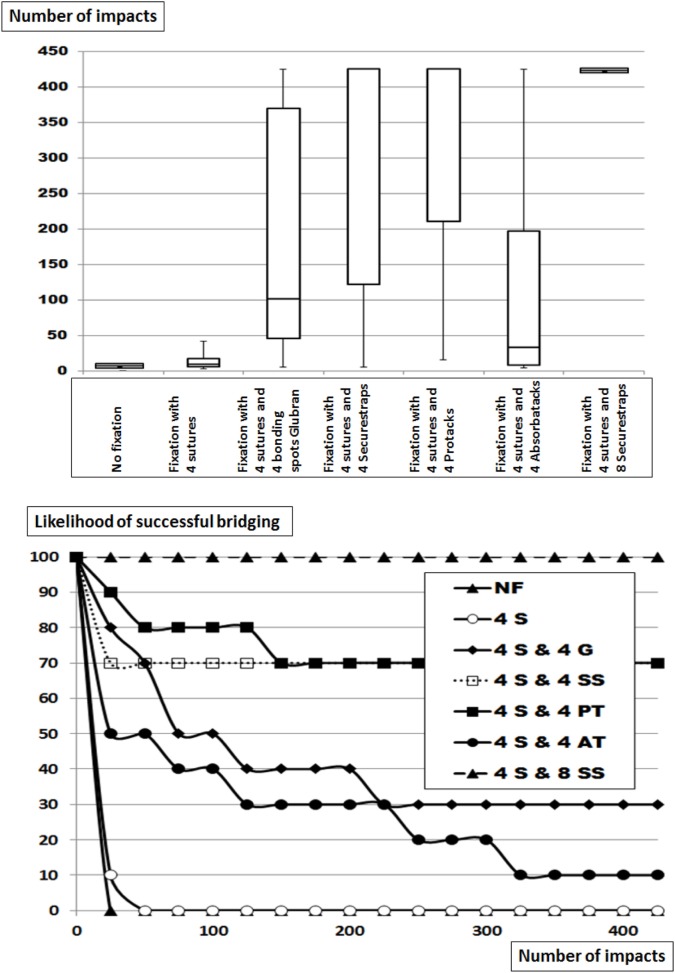
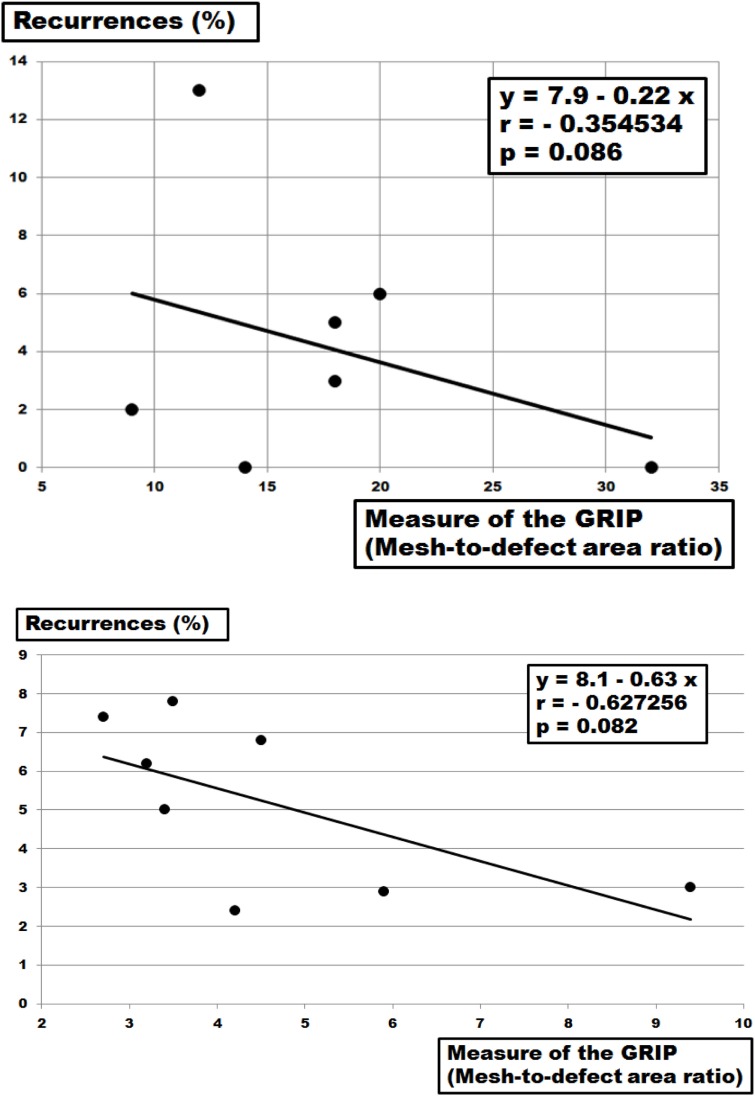
Recurrences are frequently observed after ventral hernia repair. Based on clinical data, the mesh-defect area ratio (MDAR) can lead to lower recurrence rates. Using dynamic intermittent strain (DIS) in a pig tissue model, MDAR can be modified to give a measure called grip to better assess the mechanical stability of ventral hernia repair. The focus of this experimental study is to assess the different aspects of mesh overlap (OL) and fixation only in bridging repair of ventral hernias. DIS mimics coughing actions in an model with the repetition of submaximal impacts delivered a hydraulically driven plastic containment. Tissue derived from pig bellies simulates a ventral hernia with varying defect sizes. MDAR is calculated from the hernia orifice and the mesh OL. Commercially available meshes were strengthened with glue, tacks, and sutures to bridge the defects. The reconstructions are strained with up to 425 dynamic impacts. The grip of each repair is assessed using MDAR modified by the strength of the fixation. The DIS classification is based on bridging of a 5 cm ventral hernia orifice with an OL of 5 cm in a sublay position. The classification discriminates meshes properties upon DIS strain. MDAR is calculated to be 9 under these conditions. Decreasing the OL or increasing the hernia orifice reduces MDAR to numbers below 9. MDAR is modified to reach GRIP. Closure of the peritoneum adds about 4 to the grip given by MDAR. The multiplying factor of a transmural suture or one tack of Securestrap or Protack is 0.5 times the number of tacks applied. The multiplier given by a bonding spot of Glubran is similar to that of an Absorbatack being 0.33. Plotting the likelihood of a bridging repair to survive more than 400 DIS impacts versus the grip estimated from the factors given above, the grip to be passed for a durable repair is 10 for Parietex Progrip, and Dynamesh Cicat and 25 for Dynamesh IPOM. Clinical data previously published can be reculculated to assess MDAR and permit an estimation of the grip of the reconstruction. In these recalculations, a correlation between MDAR and long-term recurrence rates is found. A dimensionless number called grip can be calculated. The grip can be modified by fixation in a reproducible way. A higher grip can improve the durability of ventral hernia repair. We believe that a higher grip leads to lower recurrence rates in the clinical setting.
腹疝修补术后复发情况屡见不鲜。根据临床数据,网片缺损面积比(MDAR)可降低复发率。在猪组织模型中使用动态间歇性应变(DIS),可对MDAR进行修正,得出一种名为抓地力的测量指标,以更好地评估腹疝修补术的机械稳定性。本实验研究的重点是仅在腹疝的桥接修补中评估网片重叠(OL)和固定的不同方面。DIS在一个模型中模拟咳嗽动作,通过液压驱动的塑料容器重复施加次最大冲击力。取自猪腹部的组织模拟不同大小缺损的腹疝。MDAR由疝孔和网片OL计算得出。使用胶水、钉和缝线加强市售网片以桥接缺损。重建后的组织承受多达425次动态冲击。使用经固定强度修正的MDAR评估每次修补的抓地力。DIS分类基于在腹膜前位置用5厘米的OL桥接5厘米的腹疝孔。该分类可区分DIS应变时网片的特性。在这些条件下计算得出MDAR为9。减小OL或增大疝孔会使MDAR降至9以下。对MDAR进行修正以得出抓地力。缝合腹膜可使MDAR给出的抓地力增加约4。透壁缝线或一根Securestrap或Protack钉的倍增系数是所用钉数量的0.5倍。Glubran粘结点给出的倍增系数与Absorbatack的相似,为0.33。绘制桥接修补在超过400次DIS冲击下存活的可能性与根据上述因素估算的抓地力的关系图,对于Parietex Progrip和Dynamesh Cicat,持久修补所需通过的抓地力为10,对于Dynamesh IPOM为25。可以重新计算先前发表的临床数据以评估MDAR,并估算重建的抓地力。在这些重新计算中,发现MDAR与长期复发率之间存在相关性。可计算出一个名为抓地力的无量纲数。抓地力可通过固定以可重复的方式进行修正。更高的抓地力可提高腹疝修补术的耐久性。我们认为在临床环境中,更高的抓地力会导致更低的复发率。