Kelly Blane C, Constantinescu David S, Pavlis William, Vap Alexander R
Virginia Commonwealth University, Richmond, Virginia, U.S.A.
University of Miami, Miami, Florida, U.S.A.
Arthrosc Sports Med Rehabil. 2021 Oct 13;3(6):e1865-e1871. doi: 10.1016/j.asmr.2021.09.001. eCollection 2021 Dec.
To evaluate whether fellowship training had an effect on the practice pattern and complication rates among Part II examinees of the American Board of Orthopaedic Surgery (ABOS) for rotator cuff repair (RCR) from 2007-2017.
The ABOS database was queried for arthroscopic (Current Procedural Terminology [CPT] code 29827) and open/mini-open (CPT codes: 23410, 23412) RCR performed from 2007-2017. Excluded were procedures that did not included CPT codes 29827, 23410, 23412. A comparison between arthroscopic and open/mini-open use as well as self-reported complications were assessed based on recorded fellowship training.
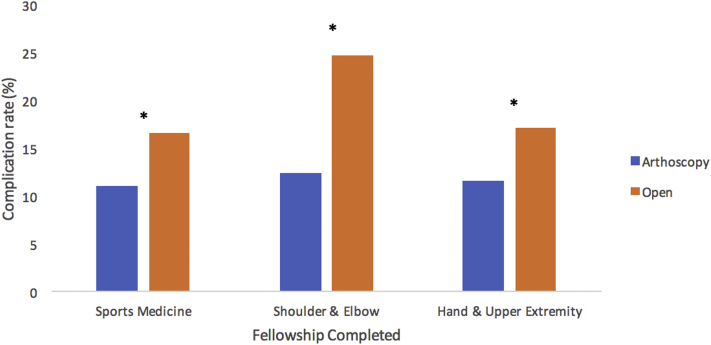
A total of 31,907 RCR were reported over the past 10 years (2007-2017). The percentage of RCR procedures performed using arthroscopic technique vs open/mini-open varied among surgeons who completed one fellowship: Sports Medicine (92.5 % arthroscopy; 7.5 % mini/open), Shoulder & Elbow (91.3 % arthroscopy; 8.7% mini/open), and Hand & Upper Extremity (69.6 % arthroscopy; 30.4 % open). Total complication rates varied among surgeons who completed one fellowship: Sports Medicine (11.5 %), Shoulder & Elbow (13.5 %), and Hand & Upper Extremity (13.4 %). Surgeons completing one fellowship in either Sports Medicine, Shoulder & Elbow, Hand & Upper Extremity all reported significantly lower complication rates using arthroscopic over mini/open technique ( < .001).
Among ABOS Part II examinees completing a Sports Medicine, Shoulder and Elbow or Hand and Upper Extremity fellowship, Sports Medicine trained surgeons had significantly greater rates of performing arthroscopic over open RCR and significantly lower self-reported intraoperative complication rates.
Understanding the effects of fellowship training may guide mentors and future trainees.
评估2007年至2017年期间,专科培训对美国骨科医师协会(ABOS)第二部分肩袖修复(RCR)考生的手术方式及并发症发生率是否有影响。
查询ABOS数据库中2007年至2017年期间进行的关节镜下(当前操作术语[CPT]代码29827)及开放/迷你开放(CPT代码:23410、23412)RCR手术。排除未包含CPT代码29827、23410、23412的手术。根据记录的专科培训情况,评估关节镜手术与开放/迷你开放手术的使用情况以及自我报告的并发症之间的差异。
在过去10年(2007年至2017年)共报告了31907例RCR手术。完成一项专科培训的外科医生中,采用关节镜技术与开放/迷你开放技术进行RCR手术的比例各不相同:运动医学(92.5%关节镜手术;7.5%迷你/开放手术)、肩肘外科(91.3%关节镜手术;8.7%迷你/开放手术)以及手与上肢外科(69.6%关节镜手术;30.4%开放手术)。完成一项专科培训的外科医生的总并发症发生率各不相同:运动医学(11.5%)、肩肘外科(13.5%)以及手与上肢外科(13.4%)。完成运动医学、肩肘外科或手与上肢外科专科培训的外科医生均报告,与迷你/开放技术相比,采用关节镜技术的并发症发生率显著更低(<0.001)。
在完成运动医学、肩肘或手与上肢专科培训的ABOS第二部分考生中,接受运动医学培训的外科医生进行关节镜下RCR手术的比例显著高于开放手术,且自我报告的术中并发症发生率显著更低。
了解专科培训的效果可能会对带教老师和未来的学员有所指导。