Kurul Şerife, Simons Sinno H P, Ramakers Christian R B, De Rijke Yolanda B, Kornelisse René F, Kroon André A, Reiss Irwin K M, Taal H Rob
Department of Pediatrics, Division Neonatology, Erasmus MC, University Medical Center-Sophia Children's Hospital, Rotterdam, The Netherlands.
Department of Clinical Chemistry, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
Crit Care Explor. 2021 Dec 2;3(12):e0585. doi: 10.1097/CCE.0000000000000585. eCollection 2021 Dec.
Late-onset neonatal sepsis is a major complication in preterm neonates. Early identification of the type of infection could help to improve therapy and outcome depending on the suspected microorganism by tailoring antibiotic treatment to the individual patient based on the predicted organism. Results of blood cultures may take up to 2 days or may remain negative in case of clinical sepsis. Chemical biomarkers may show different patterns in response to different type of microorganisms.
The aim of this study was to develop, as a proof of concept, a simple classification tree algorithm using readily available information from biomarkers to show that biomarkers can potentially be used in discriminating in the type of infection in preterm neonates suspected of late-onset neonatal sepsis.
A total of 509 suspected late-onset neonatal sepsis episodes in neonates born before less than 32 weeks of gestation were analyzed. To examine model performance, 70% of the original dataset was randomly selected as a derivation cohort ( = 356; training dataset).
The remaining 30% of the original dataset was used as a validation cohort ( = 153; test dataset).
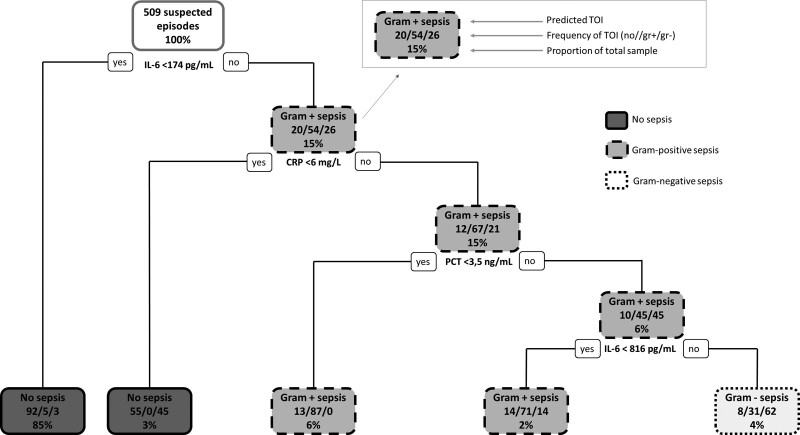
A classification tree prediction algorithm was applied to predict type of infection (defined as no/Gram-positive/Gram-negative sepsis).
Suspected late-onset neonatal sepsis episodes were classified as no sepsis (80.8% [ = 411]), Gram-positive sepsis (13.9% [ = 71]), and Gram-negative sepsis (5.3% [ = 27]). When the derived classification tree was applied to the test cohort, the overall accuracy was 87.6% (95% CI, 81.3-92.4; = 0.008). The classification tree demonstrates that interleukin-6 is the most important differentiating biomarker and C-reactive protein and procalcitonin help to further differentiate.
We have developed and internally validated a simple, clinically relevant model to discriminate patients with different types of infection at moment of onset. Further research is needed to prospectively validate this in a larger population and assess whether adaptive antibiotic regimens are feasible.
迟发性新生儿败血症是早产儿的主要并发症。早期识别感染类型有助于根据疑似微生物改善治疗和预后,即根据预测的病原体为个体患者量身定制抗生素治疗方案。血培养结果可能需要长达2天,或者在临床败血症的情况下可能仍为阴性。化学生物标志物可能因不同类型的微生物而呈现不同模式。
本研究的目的是作为概念验证,开发一种简单的分类树算法,利用生物标志物的现成信息,以表明生物标志物可潜在地用于区分疑似迟发性新生儿败血症的早产儿的感染类型。
对总共509例孕周小于32周出生的新生儿疑似迟发性新生儿败血症发作进行了分析。为了检验模型性能,将原始数据集的70%随机选择作为推导队列(n = 356;训练数据集)。
原始数据集的其余30%用作验证队列(n = 153;测试数据集)。
应用分类树预测算法预测感染类型(定义为无/革兰氏阳性/革兰氏阴性败血症)。
疑似迟发性新生儿败血症发作被分类为无败血症(80.8% [n = 411])、革兰氏阳性败血症(13.9% [n = 71])和革兰氏阴性败血症(5.3% [n = 27])。当将推导的分类树应用于测试队列时,总体准确率为87.6%(95%CI,81.3 - 92.4;p = 0.008)。分类树表明白细胞介素-6是最重要的鉴别生物标志物,C反应蛋白和降钙素原有助于进一步鉴别。
我们已经开发并在内部验证了一种简单的、与临床相关的模型,用于在发病时区分不同类型感染的患者。需要进一步研究以在更大人群中进行前瞻性验证,并评估适应性抗生素治疗方案是否可行。