Eichberger Julia, Resch Elisabeth, Resch Bernhard
Research Unit for Neonatal Infectious Diseases and Epidemiology, Medical University of Graz, Graz, Austria.
Division of Neonatology, Department of Pediatrics and Adolescent Medicine, Medical University of Graz, Graz, Austria.
Front Pediatr. 2022 Mar 8;10:840288. doi: 10.3389/fped.2022.840288. eCollection 2022.
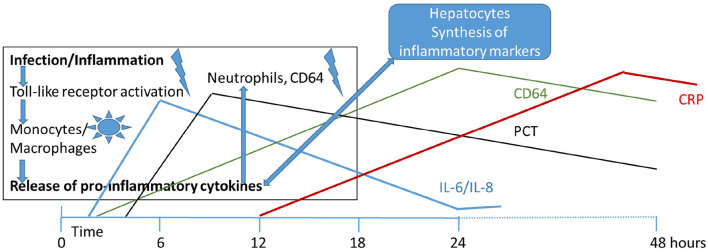
This is a narrative review on the role of biomarkers in the diagnosis of neonatal sepsis. We describe the difficulties to obtain standardized definitions in neonatal sepsis and discuss the limitations of published evidence of cut-off values and their sensitivities and specificities. Maternal risk factors influence the results of inflammatory markers as do gestational age, the time of sampling, the use of either cord blood or neonatal peripheral blood, and some non-infectious causes. Current evidence suggests that the use of promising diagnostic markers such as CD11b, CD64, IL-6, IL-8, PCT, and CRP, either alone or in combination, might enable clinicians discontinuing antibiotics confidently within 24-48 h. However, none of the current diagnostic markers is sensitive and specific enough to support the decision of withholding antibiotic treatment without considering clinical findings. It therefore seems to be justified that antibiotics are often initiated in ill term and especially preterm infants. Early markers like IL-6 and later markers like CRP are helpful in the diagnosis of neonatal sepsis considering the clinical aspect of the neonate, the gestational age, maternal risk factors and the time (age of the neonate regarding early-onset sepsis) of blood sampling.
这是一篇关于生物标志物在新生儿败血症诊断中作用的叙述性综述。我们描述了在新生儿败血症中获得标准化定义的困难,并讨论了已发表的截断值证据及其敏感性和特异性的局限性。母体风险因素会影响炎症标志物的结果,胎龄、采样时间、脐带血或新生儿外周血的使用以及一些非感染性原因也会产生影响。目前的证据表明,单独或联合使用有前景的诊断标志物,如CD11b、CD64、IL-6、IL-8、降钙素原(PCT)和C反应蛋白(CRP),可能会使临床医生在24至48小时内自信地停用抗生素。然而,目前没有一种诊断标志物足够敏感和特异,能够在不考虑临床发现的情况下支持停止抗生素治疗的决定。因此,对于足月儿尤其是早产儿,经常开始使用抗生素似乎是合理的。考虑到新生儿的临床情况、胎龄、母体风险因素以及采血时间(早发型败血症时新生儿的年龄),像IL-6这样的早期标志物和像CRP这样的后期标志物有助于新生儿败血症的诊断。