Université de Paris, 75006, Paris, France.
Radiology Department, Assistance Publique-Hôpitaux de Paris (AP-HP), Hôpital Cochin, Service de Radiologie27 rue du Faubourg Saint Jacques, 75014, Paris, France.
Eur Radiol. 2022 Apr;32(4):2704-2712. doi: 10.1007/s00330-021-08377-9. Epub 2022 Jan 7.
To identify which level of D-dimer would allow the safe exclusion of pulmonary embolism (PE) in COVID-19 patients presenting to the emergency department (ED).
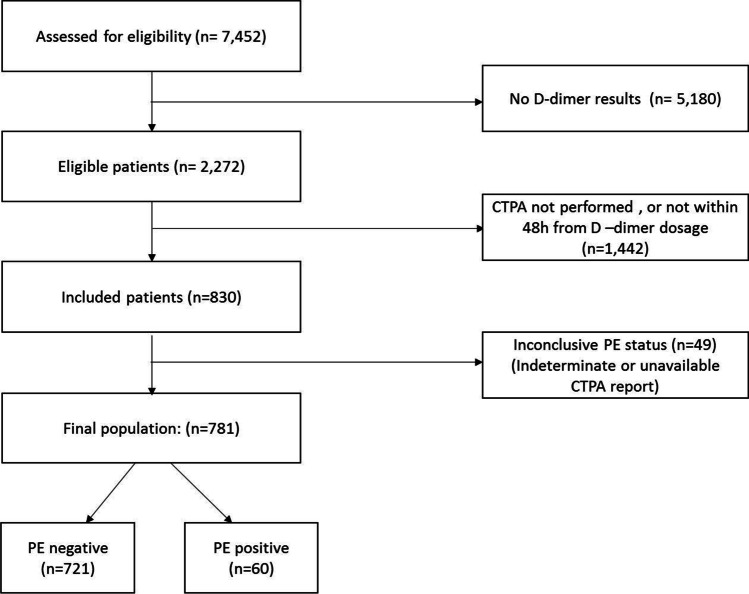
This retrospective study was conducted on the COVID database of Assistance Publique - Hôpitaux de Paris (AP-HP). COVID-19 patients who presented at the ED of AP-HP hospitals between March 1 and May 15, 2020, and had CTPA following D-dimer dosage within 48h of presentation were included. The D-dimer sensitivity, specificity, and positive and negative predictive values were calculated for different D-dimer thresholds, as well as the false-negative and failure rates, and the number of CTPAs potentially avoided.
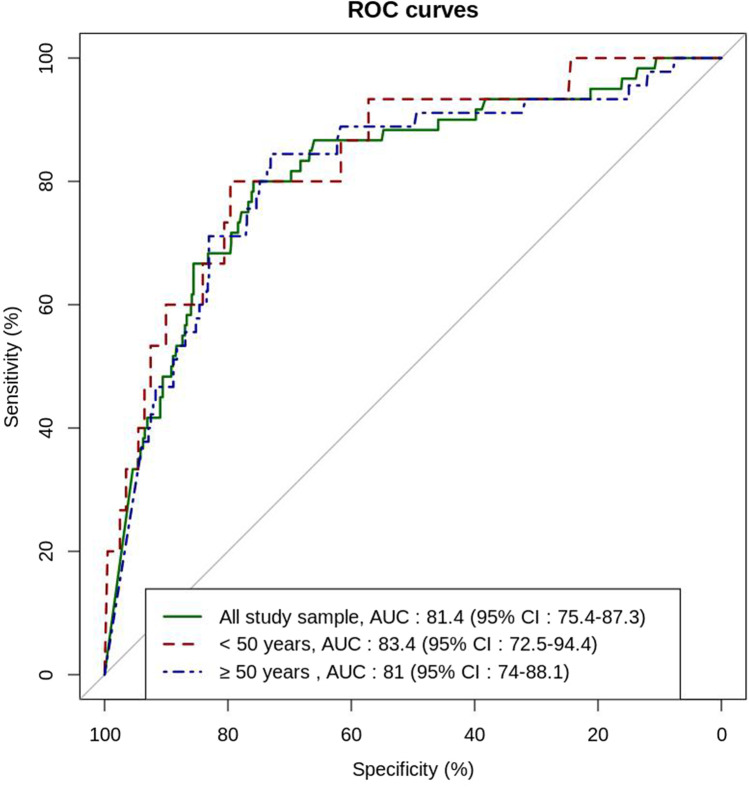
A total of 781 patients (mean age 62.0 years, 53.8% men) with positive RT-PCR for SARS-Cov-2 were included and 60 of them (7.7%) had CTPA-confirmed PE. Their median D-dimer level was significantly higher than that of patients without PE (4,013 vs 1,198 ng·mL, p < 0.001). Using 500 ng·mL, or an age-adjusted cut-off for patients > 50 years, the sensitivity and the NPV were above 90%. With these thresholds, 17.1% and 31.5% of CTPAs could have been avoided, respectively. Four of the 178 patients who had a D-dimer below the age-adjusted cutoff had PE, leading to an acceptable failure rate of 2.2%. Using higher D-dimer cut-offs could have avoided more CTPAs, but would have lowered the sensitivity and increased the failure rate.
The same D-Dimer thresholds as those validated in non-COVID outpatients should be used to safely rule out PE.
• The median D-dimer level was significantly higher in COVID-19 patients with PE as compared to those without PE (4,013 ng·mL vs 1,198 ng·mL respectively, p < 0.001). • Using 500 ng·mL, or an age-adjusted D-dimer cut-off to exclude pulmonary embolism, the sensitivity and negative predictive value were above 90%. • Higher cut-offs would lead to a reduction in the sensitivity below 85% and an increase in the failure rate, especially for patients under 50 years.
确定 D-二聚体的何种水平可安全排除 COVID-19 患者急诊就诊时发生的肺栓塞(PE)。
这是一项回顾性研究,纳入了巴黎公立医院集团(AP-HP)COVID 数据库中的患者。2020 年 3 月 1 日至 5 月 15 日期间在 AP-HP 医院急诊就诊且 D-二聚体检测后 48 小时内行 CTPA 的 COVID-19 患者。计算不同 D-二聚体截断值的 D-二聚体敏感度、特异度、阳性预测值和阴性预测值,以及假阴性率和漏诊率,以及可能避免的 CTPA 数量。
共纳入 781 例 SARS-CoV-2 阳性的 RT-PCR 检测患者(平均年龄 62.0 岁,53.8%为男性),其中 60 例(7.7%)患者 CTPA 确诊为 PE。与无 PE 患者相比,这些患者的中位 D-二聚体水平显著升高(4013 比 1198ng·mL,p<0.001)。使用 500ng·mL 或年龄校正截断值(>50 岁患者)时,敏感度和阴性预测值均>90%。采用这些截断值,分别可避免 17.1%和 31.5%的 CTPA。在 D-二聚体低于年龄校正截断值的 178 例患者中,有 4 例患者发生 PE,漏诊率为 2.2%,可接受。采用更高的 D-二聚体截断值可能会避免更多的 CTPA,但会降低敏感度并增加漏诊率。
应采用与非 COVID 门诊患者中验证的相同 D-二聚体截断值来安全排除 PE。
COVID-19 合并 PE 患者的中位 D-二聚体水平显著高于无 PE 患者(分别为 4013ng·mL 和 1198ng·mL,p<0.001)。
使用 500ng·mL 或年龄校正 D-二聚体截断值排除 PE 时,敏感度和阴性预测值均>90%。
较高的截断值会导致敏感度降至 85%以下,漏诊率增加,尤其是 50 岁以下患者。