Department of Epidemiology, Tulane University School of Public Health and Tropical Medicine, and Tulane University Translational Science Institute, New Orleans, Louisiana (J.D.B., K.T.M.).
Department of Epidemiology, Tulane University School of Public Health and Tropical Medicine, and Tulane University Translational Science Institute, New Orleans, Louisiana, and Department of Biostatistics, Epidemiology, and Informatics, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania (A.H.A.).
Ann Intern Med. 2022 Mar;175(3):305-313. doi: 10.7326/M21-2928. Epub 2022 Jan 11.
New estimated glomerular filtration rate (eGFR) equations removed race adjustment, but the impact of its removal on prediction of end-stage kidney disease (ESKD) is unknown.
To compare the ESKD prediction performance of different eGFR equations.
Observational, prospective cohort study.
7 U.S. clinical centers.
3873 participants with chronic kidney disease (CKD) from the CRIC (Chronic Renal Insufficiency Cohort) Study contributing 13 902 two-year risk periods.
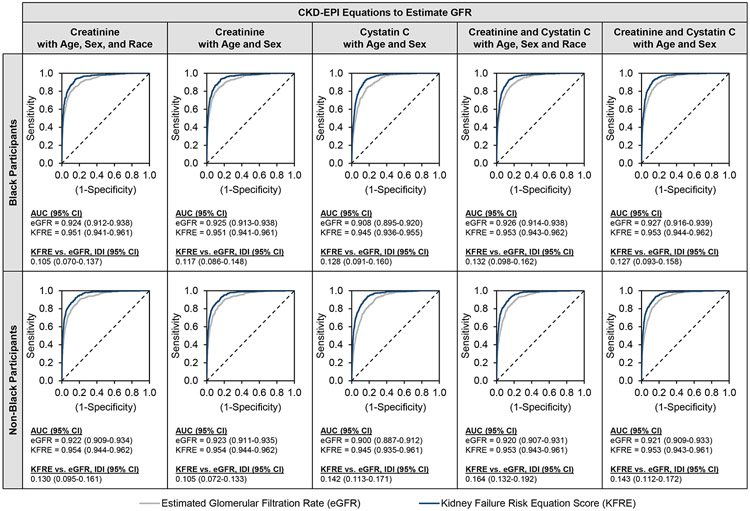
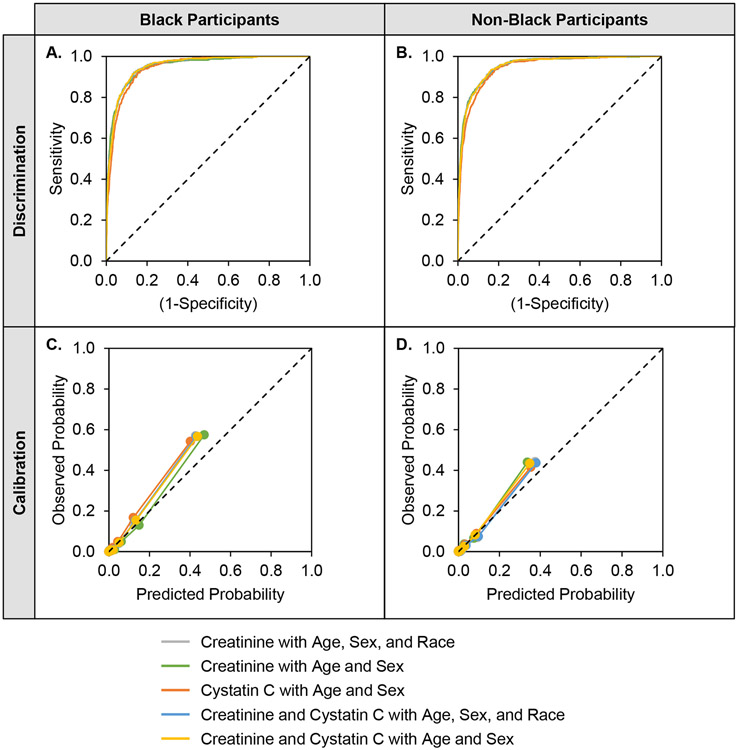
ESKD was defined as initiation of dialysis or transplantation. eGFR was calculated using 5 Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations based on serum creatinine and/or cystatin C, with or without race adjustment. The predicted 2-year risk for ESKD was calculated using the 4-variable Kidney Failure Risk Equation (KFRE). We evaluated the prediction performance of eGFR equations and the KFRE score using discrimination and calibration analyses.
During a maximum 16 years of follow-up, 856 participants developed ESKD. Across all eGFR equations, the KFRE score was superior for predicting 2-year incidence of ESKD compared with eGFR alone (area under the curve ranges, 0.945 to 0.954 vs. 0.900 to 0.927). Prediction performance of KFRE scores using different eGFR equations was similar, but the creatinine equation without race adjustment improved calibration among Black participants. Among all participants, compared with an eGFR less than 20 mL/min/1.73 m, a KFRE score greater than 20% had similar specificity for predicting 2-year ESKD risk (ranges, 0.94 to 0.97 vs. 0.95 to 0.98) but higher sensitivity (ranges, 0.68 to 0.78 vs. 0.42 to 0.66).
Data are solely from the United States.
The KFRE score better predicts 2-year risk for ESKD compared with eGFR alone, regardless of race adjustment. The creatinine equation with age and sex may improve calibration among Black patients. A KFRE score greater than 20% showed high specificity and sensitivity for predicting 2-year risk for ESKD.
National Institutes of Health.
新的估计肾小球滤过率(eGFR)方程去除了种族调整,但它对终末期肾病(ESKD)预测的影响尚不清楚。
比较不同 eGFR 方程在 ESKD 预测中的性能。
观察性、前瞻性队列研究。
美国 7 个临床中心。
来自 CRIC(慢性肾功能不全队列)研究的 3873 名慢性肾脏病(CKD)患者,共贡献了 13902 个两年风险期。
ESKD 的定义为开始透析或移植。使用基于血清肌酐和/或胱抑素 C 的 5 种慢性肾脏病流行病学合作组(CKD-EPI)方程计算 eGFR,其中包括或不包括种族调整。使用 4 变量肾功能衰竭风险方程(KFRE)计算 ESKD 的 2 年预测风险。我们使用区分和校准分析评估 eGFR 方程和 KFRE 评分的预测性能。
在最长 16 年的随访期间,856 名参与者发生 ESKD。在所有 eGFR 方程中,KFRE 评分在预测 2 年 ESKD 发生率方面优于单独的 eGFR(曲线下面积范围,0.945 至 0.954 与 0.900 至 0.927)。使用不同 eGFR 方程的 KFRE 评分的预测性能相似,但无种族调整的肌酐方程改善了黑人参与者的校准。在所有参与者中,与 eGFR 小于 20 mL/min/1.73 m 相比,KFRE 评分大于 20%对预测 2 年 ESKD 风险具有相似的特异性(范围,0.94 至 0.97 与 0.95 至 0.98),但敏感性更高(范围,0.68 至 0.78 与 0.42 至 0.66)。
数据仅来自美国。
无论种族调整如何,KFRE 评分均优于单独的 eGFR 更好地预测 2 年 ESKD 风险。包含年龄和性别的肌酐方程可能会改善黑人患者的校准。KFRE 评分大于 20%对预测 2 年 ESKD 风险具有高特异性和敏感性。
美国国立卫生研究院。