Université de Paris, Inserm U1153, Epidemiology of Ageing and Neurodegenerative Diseases, Paris, France
Université de Paris, Inserm U1153, Epidemiology of Ageing and Neurodegenerative Diseases, Paris, France.
BMJ. 2022 Feb 2;376:e068005. doi: 10.1136/bmj-2021-068005.
To examine the association of midlife and late life multimorbidity, including severity of multimorbidity, with incident dementia.
Prospective cohort study.
Civil service departments in London (Whitehall II study, study inception in 1985-88).
10 095 participants, aged 35 to 55 at baseline.
Incident dementia at follow-up between 1985 and 2019. Cause specific Cox proportional hazards regression was used to examine the association of multimorbidity overall and at age 55, 60, 65, and 70 with subsequent dementia, taking into account the competing risk of death.
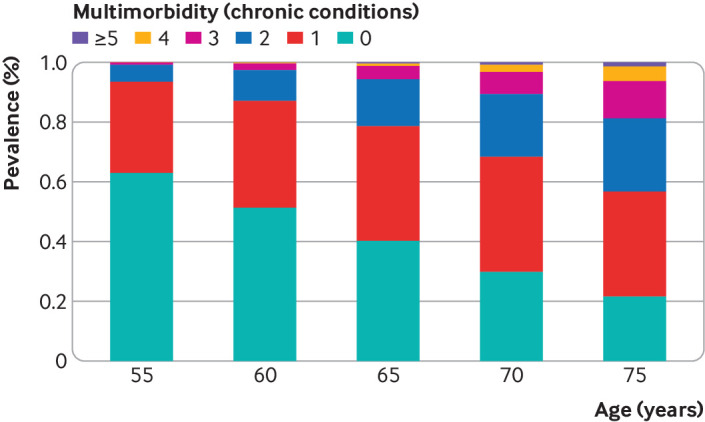
The prevalence of multimorbidity (≥2 chronic diseases) was 6.6% (655/9937) at age 55 and 31.7% (2464/7783) at age 70; 639 cases of incident dementia occurred over a median follow-up of 31.7 years. After adjustment for sociodemographic factors and health behaviours, multimorbidity at age 55 was associated with subsequent risk of dementia (difference in incidence rate per 1000 person years 1.56, 95% confidence interval 0.62 to 2.77; hazard ratio 2.44, 95% confidence interval 1.82 to 3.26). The association weakened progressively with older age at onset of multimorbidity. At age 65, onset of multimorbidity before age 55 was associated with 3.86 (1.80 to 6.52) per 1000 person years higher incidence of dementia (hazard ratio 2.46, 1.80 to 2.26) and onset between 60 and 65 was associated with 1.85 (0.64 to 3.39) per 1000 person years higher incidence (1.51, 1.16 to 1.97). Severity of multimorbidity (≥3 chronic diseases) at age 55 was associated with a 5.22 (1.14 to 11.95) per 1000 person years higher incidence of dementia (hazard ratio 4.96, 2.54 to 9.67); the same analyses at age 70 showed 4.49 (2.33 to 7.19) per 1000 person years higher incidence (1.65, 1.25 to 2.18).
Multimorbidity, particularly when onset is in midlife rather than late life, has a robust association with subsequent dementia. The increasingly younger age at onset of multimorbidity makes prevention of multimorbidity in people with a first chronic disease important.
探讨中年和晚年多种疾病的发生情况,包括多种疾病的严重程度与痴呆症发病的关系。
前瞻性队列研究。
伦敦公务员部门(白厅 II 研究,研究始于 1985-1988 年)。
10095 名参与者,基线时年龄在 35 至 55 岁之间。
1985 年至 2019 年随访期间的痴呆症发病情况。采用多因素 Cox 比例风险回归分析,在考虑死亡竞争风险的情况下,分析总体和 55 岁、60 岁、65 岁和 70 岁时的多种疾病与随后发生痴呆症的关系。
55 岁时,多种疾病(≥2 种慢性疾病)的患病率为 6.6%(655/9937),70 岁时为 31.7%(2464/7783);中位随访 31.7 年后发生了 639 例痴呆症病例。在调整社会人口因素和健康行为后,55 岁时的多种疾病与随后的痴呆风险相关(每 1000 人年的发病率差异为 1.56,95%置信区间为 0.62 至 2.77;风险比为 2.44,95%置信区间为 1.82 至 3.26)。这种关联随着发病年龄的增加而逐渐减弱。在 65 岁时,55 岁前发病的多种疾病与每 1000 人年增加 3.86(1.80 至 6.52)的痴呆症发病率相关(风险比为 2.46,1.80 至 2.26),60 至 65 岁发病的多种疾病与每 1000 人年增加 1.85(0.64 至 3.39)的痴呆症发病率相关(风险比为 1.51,1.16 至 1.97)。55 岁时多种疾病的严重程度(≥3 种慢性疾病)与每 1000 人年增加 5.22(1.14 至 11.95)的痴呆症发病率相关(风险比为 4.96,2.54 至 9.67);在 70 岁时进行同样的分析显示,每 1000 人年增加 4.49(2.33 至 7.19)的痴呆症发病率(风险比为 1.65,1.25 至 2.18)。
多种疾病,尤其是发病年龄从中年开始而不是晚年开始,与随后的痴呆症有很强的相关性。多种疾病发病年龄的逐渐年轻化,使得预防首次发生慢性疾病的人群发生多种疾病变得尤为重要。