Université Paris Cité, Inserm U1153, Epidemiology of Ageing and Neurodegenerative diseases, Paris, France.
Department of Epidemiology and Public Health, University College London, London, United Kingdom.
PLoS Med. 2022 Oct 18;19(10):e1004109. doi: 10.1371/journal.pmed.1004109. eCollection 2022 Oct.
Sleep duration has been shown to be associated with individual chronic diseases but its association with multimorbidity, common in older adults, remains poorly understood. We examined whether sleep duration is associated with incidence of a first chronic disease, subsequent multimorbidity and mortality using data spanning 25 years.
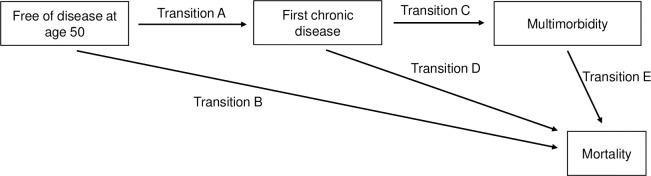
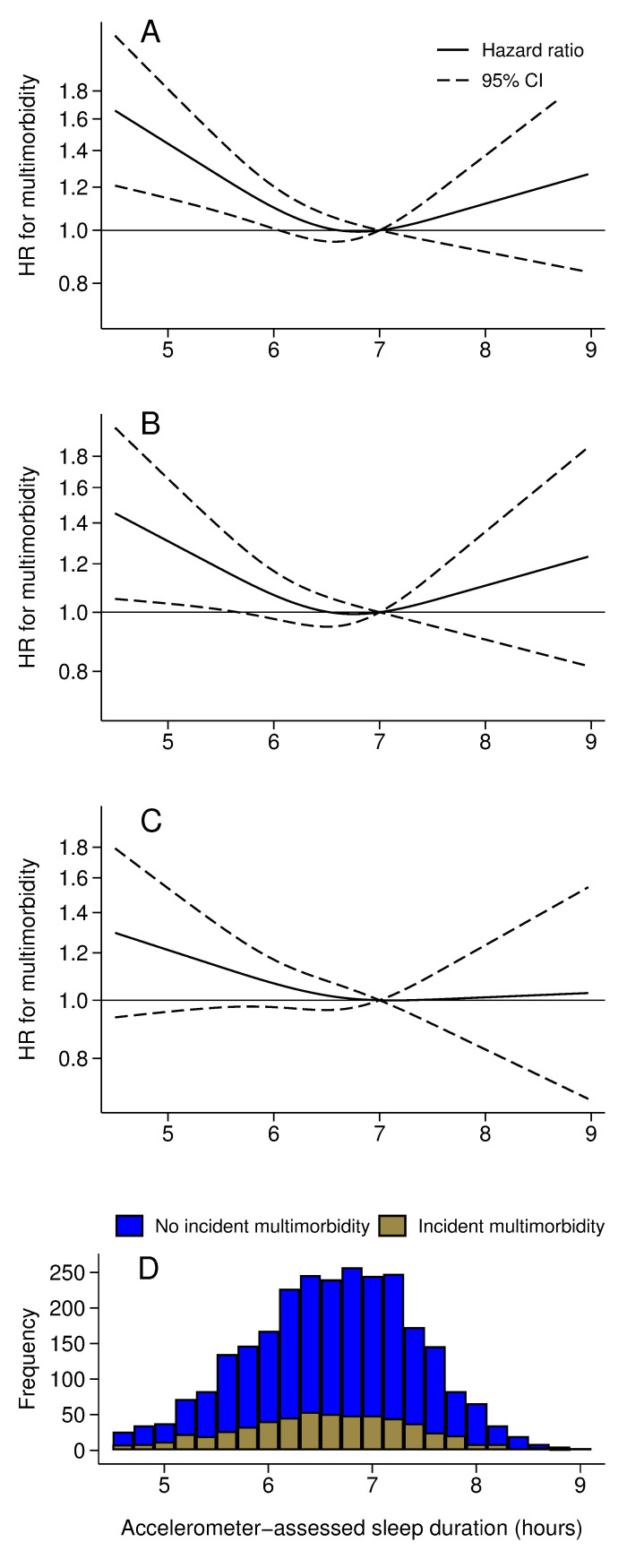
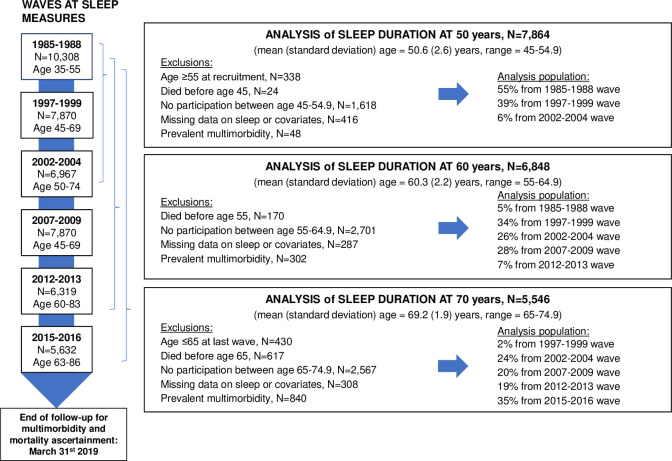
Data were drawn from the prospective Whitehall II cohort study, established in 1985 on 10,308 persons employed in the London offices of the British civil service. Self-reported sleep duration was measured 6 times between 1985 and 2016, and data on sleep duration was extracted at age 50 (mean age (standard deviation) = 50.6 (2.6)), 60 (60.3 (2.2)), and 70 (69.2 (1.9)). Incidence of multimorbidity was defined as having 2 or more of 13 chronic diseases, follow-up up to March 2019. Cox regression, separate analyses at each age, was used to examine associations of sleep duration at age 50, 60, and 70 with incident multimorbidity. Multistate models were used to examine the association of sleep duration at age 50 with onset of a first chronic disease, progression to incident multimorbidity, and death. Analyses were adjusted for sociodemographic, behavioral, and health-related factors. A total of 7,864 (32.5% women) participants free of multimorbidity had data on sleep duration at age 50; 544 (6.9%) reported sleeping ≤5 hours, 2,562 (32.6%) 6 hours, 3,589 (45.6%) 7 hours, 1,092 (13.9%) 8 hours, and 77 (1.0%) ≥9 hours. Compared to 7-hour sleep, sleep duration ≤5 hours was associated with higher multimorbidity risk (hazard ratio: 1.30, 95% confidence interval = 1.12 to 1.50; p < 0.001). This was also the case for short sleep duration at age 60 (1.32, 1.13 to 1.55; p < 0.001) and 70 (1.40, 1.16 to 1.68; p < 0.001). Sleep duration ≥9 hours at age 60 (1.54, 1.15 to 2.06; p = 0.003) and 70 (1.51, 1.10 to 2.08; p = 0.01) but not 50 (1.39, 0.98 to 1.96; p = 0.07) was associated with incident multimorbidity. Among 7,217 participants free of chronic disease at age 50 (mean follow-up = 25.2 years), 4,446 developed a first chronic disease, 2,297 progressed to multimorbidity, and 787 subsequently died. Compared to 7-hour sleep, sleeping ≤5 hours at age 50 was associated with an increased risk of a first chronic disease (1.20, 1.06 to 1.35; p = 0.003) and, among those who developed a first disease, with subsequent multimorbidity (1.21, 1.03 to 1.42; p = 0.02). Sleep duration ≥9 hours was not associated with these transitions. No association was found between sleep duration and mortality among those with existing chronic diseases. The study limitations include the small number of cases in the long sleep category, not allowing conclusions to be drawn for this category, the self-reported nature of sleep data, the potential for reverse causality that could arise from undiagnosed conditions at sleep measures, and the small proportion of non-white participants, limiting generalization of findings.
In this study, we observed short sleep duration to be associated with risk of chronic disease and subsequent multimorbidity but not with progression to death. There was no robust evidence of an increased risk of chronic disease among those with long sleep duration at age 50. Our findings suggest an association between short sleep duration and multimorbidity.
已有研究表明,睡眠时长与个体的慢性疾病有关,但在老年人中较为常见的多种慢性疾病的发生与睡眠时长之间的关系尚不清楚。本研究旨在通过随访 25 年的数据,探讨睡眠时长与首次慢性疾病的发生、随后的多种慢性疾病以及死亡率之间的关系。
本研究的数据来自前瞻性的 Whitehall II 队列研究,该研究于 1985 年在英国公务员办公室的 10308 名工作人员中开展。在 1985 年至 2016 年期间,参与者共报告了 6 次睡眠时长,在参与者 50 岁(平均年龄(标准差)= 50.6(2.6))、60 岁(60.3(2.2))和 70 岁(69.2(1.9))时提取了睡眠时长的数据。多种慢性疾病的定义为患有 13 种慢性疾病中的 2 种或以上,随访至 2019 年 3 月。采用 Cox 回归分析,分别在每个年龄组进行分析,以探讨 50 岁、60 岁和 70 岁时的睡眠时长与新发多种慢性疾病的相关性。采用多状态模型探讨 50 岁时的睡眠时长与首次慢性疾病的发生、向新发多种慢性疾病的进展以及死亡之间的关联。分析调整了社会人口统计学、行为和健康相关因素。在没有多种慢性疾病的 7864 名参与者(32.5%为女性)中,有 50 岁时睡眠时长的数据;544 名(6.9%)报告睡眠时间≤5 小时,2562 名(32.6%)报告睡眠时间为 6 小时,3589 名(45.6%)报告睡眠时间为 7 小时,1092 名(13.9%)报告睡眠时间为 8 小时,77 名(1.0%)报告睡眠时间≥9 小时。与 7 小时睡眠相比,睡眠时间≤5 小时与多种慢性疾病风险增加相关(风险比:1.30,95%置信区间:1.12 至 1.50;p<0.001)。在 60 岁(1.32,1.13 至 1.55;p<0.001)和 70 岁(1.40,1.16 至 1.68;p<0.001)时,情况也是如此。在 60 岁(1.54,1.15 至 2.06;p=0.003)和 70 岁(1.51,1.10 至 2.08;p=0.01)时,睡眠时间≥9 小时与新发多种慢性疾病相关,但在 50 岁时(1.39,0.98 至 1.96;p=0.07)则不然。在 50 岁时没有慢性疾病的 7217 名参与者(平均随访时间=25.2 年)中,4446 人患上了第一种慢性疾病,2297 人发展为多种慢性疾病,787 人随后死亡。与 7 小时睡眠相比,50 岁时睡眠时间≤5 小时与首次慢性疾病的风险增加相关(1.20,1.06 至 1.35;p=0.003),并且在那些患上第一种疾病的人中,与随后的多种慢性疾病相关(1.21,1.03 至 1.42;p=0.02)。睡眠时间≥9 小时与这些转变无关。在有现有慢性疾病的参与者中,睡眠时长与死亡率之间没有关联。研究的局限性包括长睡眠时间类别中的病例数量较少,无法对此类别得出结论,睡眠数据的自我报告性质,可能因睡眠测量时未确诊的情况而导致的潜在反向因果关系,以及非白人群体的比例较小,限制了研究结果的推广。
在这项研究中,我们观察到短睡眠时间与慢性疾病风险和随后的多种慢性疾病有关,但与进展为死亡无关。50 岁时睡眠时间较长与慢性疾病风险增加之间没有确凿的证据。我们的研究结果表明,短睡眠时间与多种慢性疾病之间存在关联。