Division of Cardiology, Department of Medicine, University of Arkansas for Medical Sciences, Little Rock, AR, USA.
Division of Cardiology, Department of Medicine, Duke University, 2301 Erwin Road, Durham, NC, USA.
Cardiovasc Diabetol. 2022 Feb 5;21(1):20. doi: 10.1186/s12933-022-01455-2.
There is uncertainty and limited data regarding initiation of sodium-glucose cotransporter 2 (SGLT2) inhibitors among patients hospitalized with acute heart failure (AHF). This systematic review and meta-analysis aim to establish the efficacy and safety of SGLT2 inhibitors initiated in patients hospitalized for AHF.
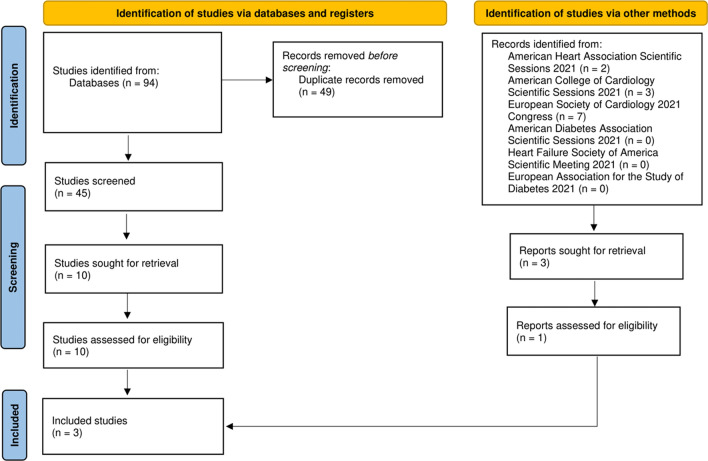
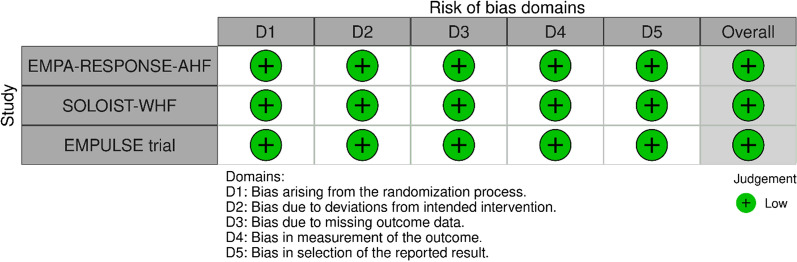
PubMed/Medline, Embase, and Cochrane library were searched using the following terms: ("sglt2" and "acute heart failure") and ("sglt2" and "worsening heart failure") from inception till November 15th, 2021 for randomized controlled trials (RCTs) comparing the efficacy and safety of initiating an SGLT2 inhibitor compared with placebo in patients with AHF. Major cardiovascular and diabetes scientific meetings in 2021 were also searched for relevant studies. Prespecified efficacy outcomes were all-cause mortality, rehospitalization for heart failure, and improvement in Kansas City Cardiomyopathy Questionnaire (KCCQ) scale score. Prespecified safety outcomes were acute kidney injury (AKI), hypotension, and hypoglycemia. Random effects odds ratio (OR) and mean difference with 95% confidence intervals (CIs) were calculated.
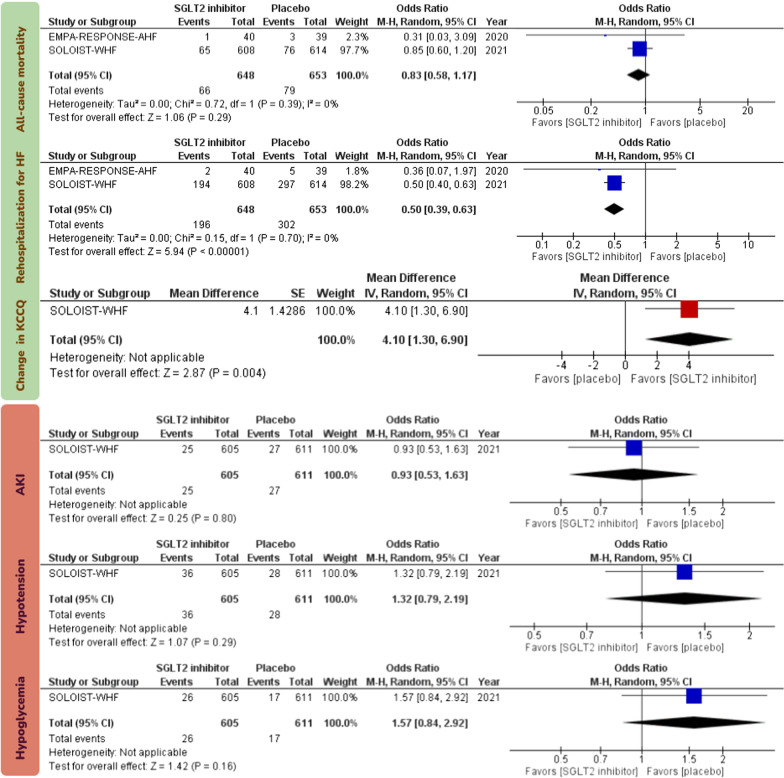
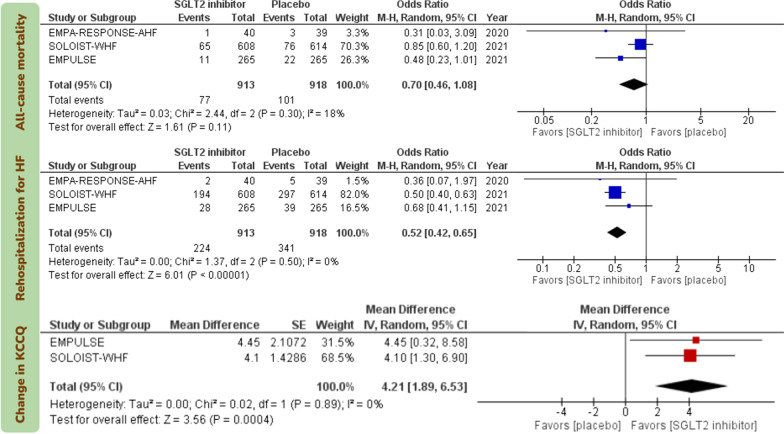
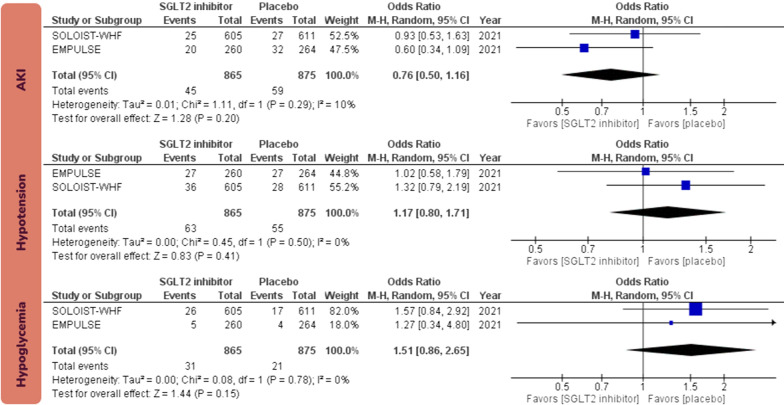
Three RCTs with a total of 1831 patients were included. Initiation of SGLT2 inhibitors in patients with AHF reduced the risk of rehospitalization for heart failure (OR 0.52; 95% CI [0.42, 0.65]) and improved Kansas City Cardiomyopathy Questionnaire scores (mean difference 4.12; 95% CI [0.1.89, 6.53]). There was no statistically significant effect for initiation of SGLT2 inhibitors in patients with AHF on all-cause mortality (OR 0.70; 95% CI [0.46, 1.08]). Initiation of SGLT2 inhibitors in patients with AHF did not increase the acute kidney injury (OR 0.76; 95% CI [0.50, 1.16]), hypotension (OR 1.17; 95% CI [0.80, 1.71]), or hypoglycemia (OR 1.51; 95% CI [0.86, 2.65]).
Initiation of SGLT2 inhibitors in patients hospitalized for AHF during hospitalization or early post-discharge (within 3 days) reduces the risk of rehospitalization for heart failure and improves patient-reported outcomes with no excess risk of adverse effects.
在因急性心力衰竭(AHF)住院的患者中,开始使用钠-葡萄糖共转运蛋白 2(SGLT2)抑制剂存在不确定性和有限的数据。本系统评价和荟萃分析旨在确定在因 AHF 住院的患者中开始使用 SGLT2 抑制剂的疗效和安全性。
使用以下术语在 PubMed/Medline、Embase 和 Cochrane 图书馆中进行搜索:(“sglt2”和“急性心力衰竭”)和(“sglt2”和“心力衰竭恶化”),从开始到 2021 年 11 月 15 日,用于比较 SGLT2 抑制剂与安慰剂在 AHF 患者中的疗效和安全性的随机对照试验(RCT)。还搜索了 2021 年主要的心血管和糖尿病科学会议的相关研究。预先规定的疗效结局为全因死亡率、因心力衰竭再次住院和堪萨斯城心肌病问卷(KCCQ)评分的改善。预先规定的安全性结局为急性肾损伤(AKI)、低血压和低血糖。计算了具有 95%置信区间(CI)的所有原因死亡率、因心力衰竭再次住院的风险比(OR)和均数差。
纳入了三项共纳入 1831 例患者的 RCT。在 AHF 患者中开始使用 SGLT2 抑制剂可降低因心力衰竭再次住院的风险(OR 0.52;95%CI [0.42, 0.65])并改善堪萨斯城心肌病问卷评分(平均差异 4.12;95%CI [0.1.89, 6.53])。在 AHF 患者中开始使用 SGLT2 抑制剂对全因死亡率无统计学显著影响(OR 0.70;95%CI [0.46, 1.08])。在 AHF 患者中开始使用 SGLT2 抑制剂不会增加急性肾损伤(OR 0.76;95%CI [0.50, 1.16])、低血压(OR 1.17;95%CI [0.80, 1.71])或低血糖(OR 1.51;95%CI [0.86, 2.65])。
在 AHF 住院期间或出院后早期(3 天内)开始使用 SGLT2 抑制剂可降低因心力衰竭再次住院的风险,并改善患者报告的结局,且无不良影响的风险增加。