Institute of Clinical Medicine, Taipei, Taiwan.
Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
Clin Gastroenterol Hepatol. 2023 Apr;21(4):960-969.e1. doi: 10.1016/j.cgh.2022.01.046. Epub 2022 Feb 4.
BACKGROUND & AIMS: The influence of nonalcoholic fatty liver disease (NAFLD) on the long-term risk of cirrhosis and hepatocellular carcinoma (HCC) in Asian populations has not been widely investigated.
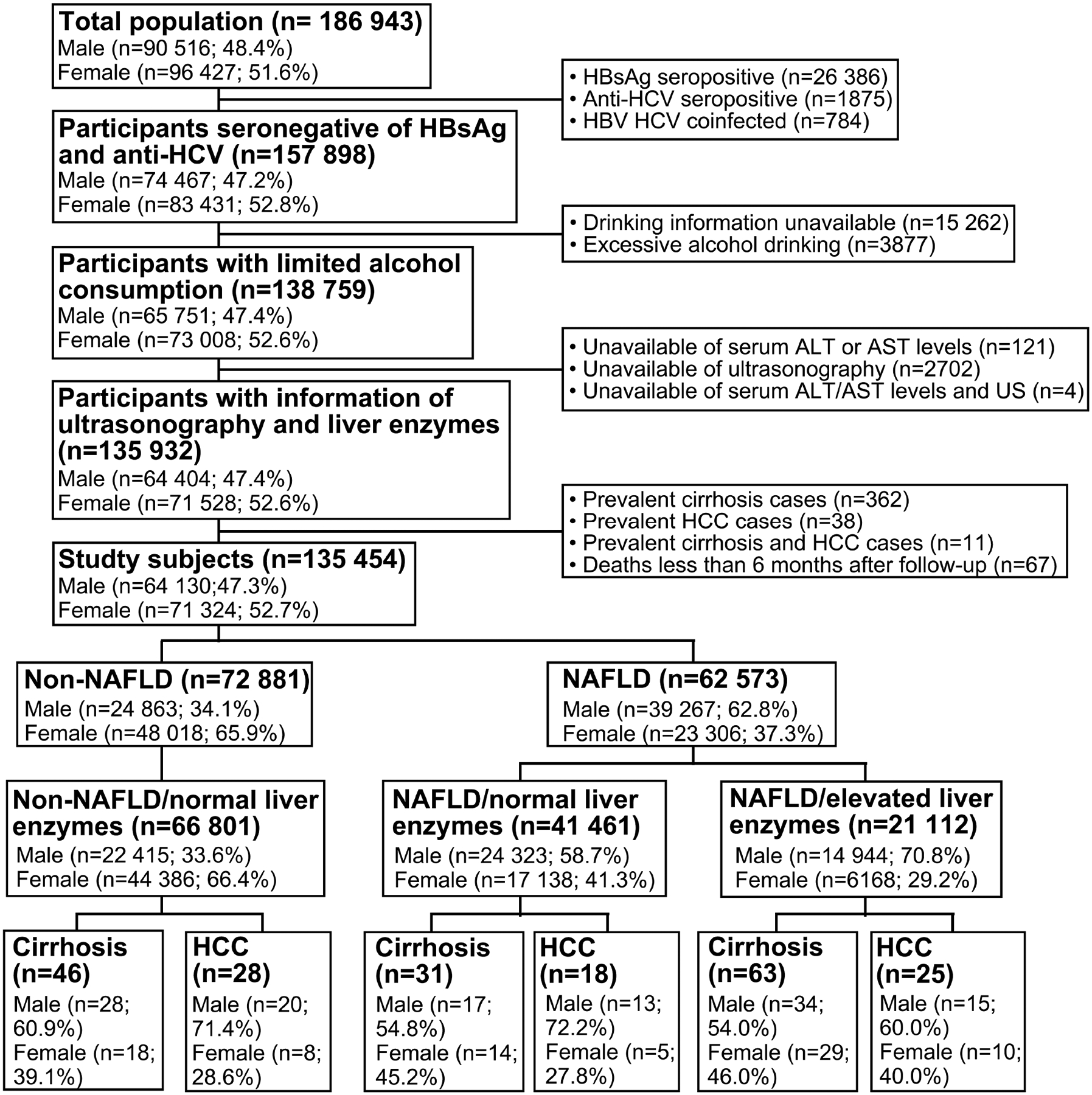
We enrolled 129,374 adults aged 30 years and older, all of whom participated in a health screening program from 2008 through 2013, were seronegative for hepatitis B surface antigen and anti-hepatitis C virus antibodies, and had limited daily alcohol consumption (<20 g/d for men and <10 g/d for women). Abdominal ultrasonography was performed to determine the presence of NAFLD. The participants were divided into the following groups: NAFLD with increased or normal liver enzyme levels, and non-NAFLD with normal liver enzyme levels. The incidences of cirrhosis and HCC were determined through computerized data linkage with nationwide registries. Cox proportional hazard models were used to estimate the hazard ratios of NAFLD on the risks of cirrhosis and HCC.
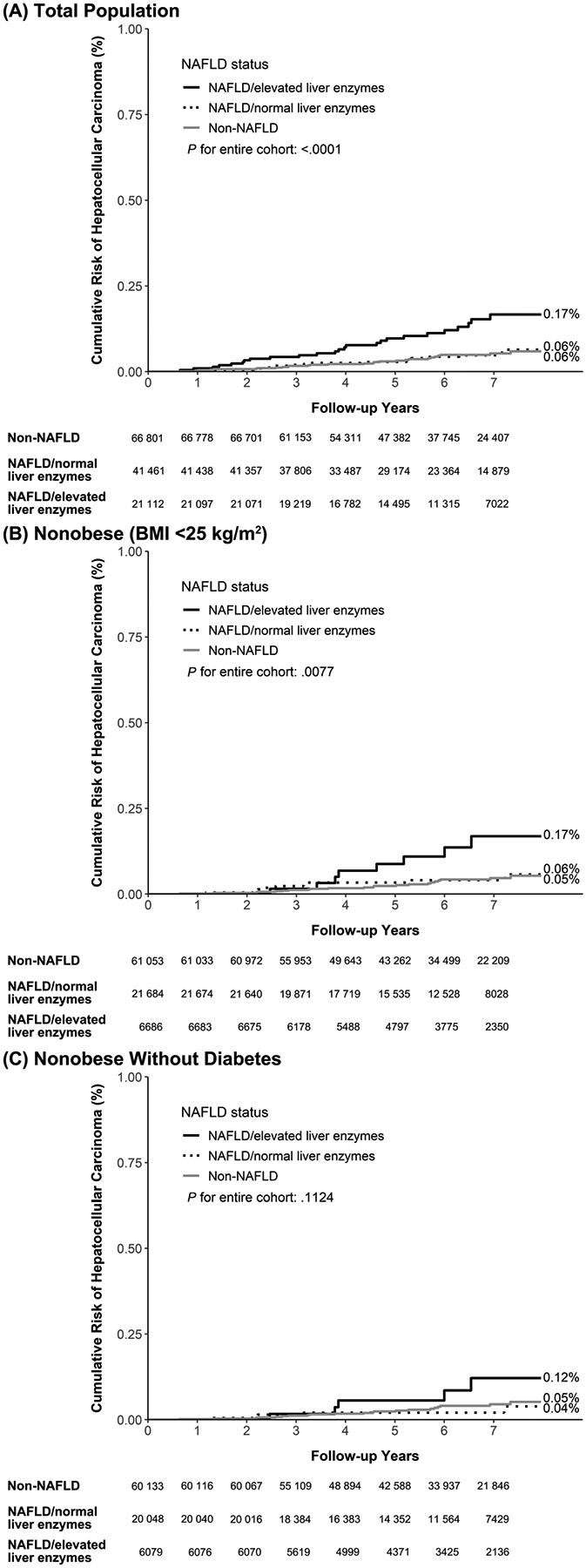
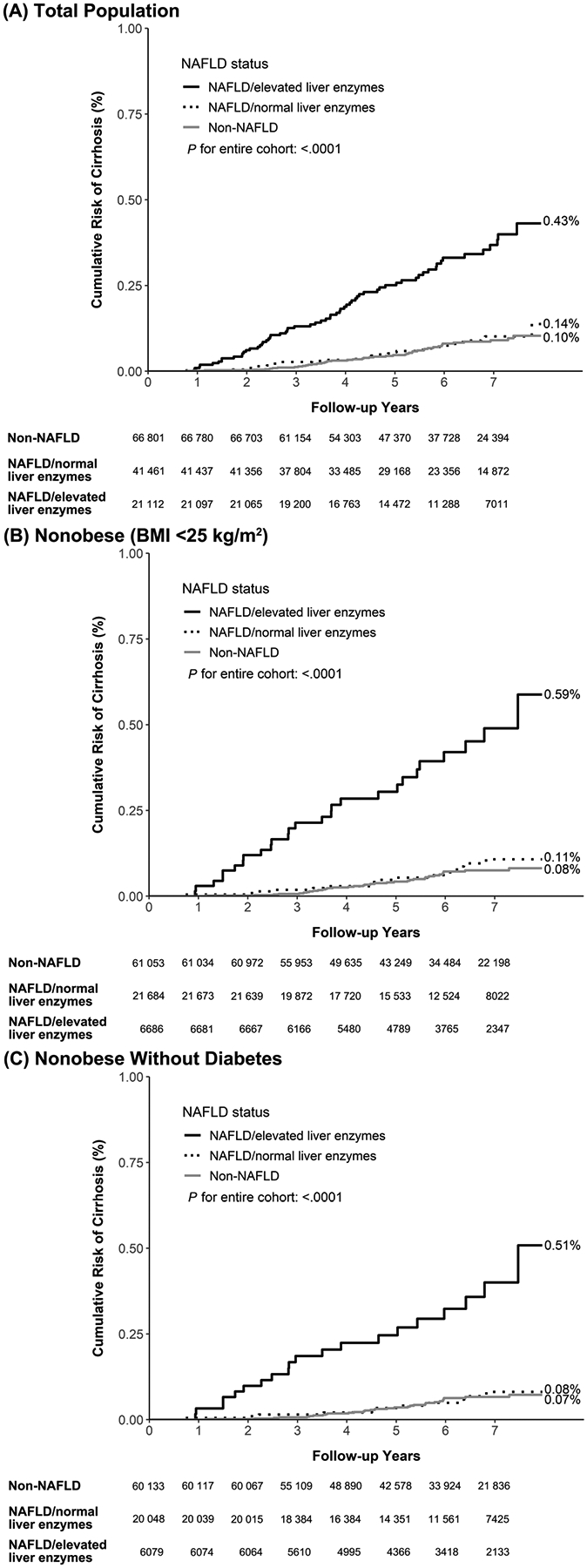
The incidence rates of cirrhosis and HCC increased as follows: non-NAFLD with normal liver enzyme levels (n = 66,801; 51%), NAFLD with normal liver enzyme levels (n = 41,461; 32%), and NAFLD with increased liver enzyme levels (n = 21,112; 16%). In the NAFLD group with increased liver enzyme levels and the NAFLD group with normal liver enzyme levels, the corresponding multivariate-adjusted hazard ratios for cirrhosis were 3.51 (95% confidence interval [CI]: 2.36-5.22) and 0.73 (95% CI: 0.46-1.16), and for HCC were 1.91 (95% CI: 1.08-3.38) and 0.57 (95% CI: 0.31-1.04), respectively, compared with the non-NAFLD group (P for trend < .001). The findings were consistent after restricting the analysis to nonobese individuals (body mass index, <25 kg/m) and nonobese individuals without diabetes (P < .05).
Individuals with NAFLD and increased liver enzyme levels showed significantly higher risks for cirrhosis and HCC and should be monitored.
非酒精性脂肪性肝病(NAFLD)对亚洲人群肝硬化和肝细胞癌(HCC)长期风险的影响尚未得到广泛研究。
我们纳入了 129374 名年龄在 30 岁及以上的成年人,他们均于 2008 年至 2013 年参加了健康筛查计划,乙型肝炎表面抗原和抗丙型肝炎病毒抗体均为阴性,且日常饮酒量有限(男性<20 g/d,女性<10 g/d)。通过腹部超声检查确定是否存在 NAFLD。参与者分为以下几组:肝酶水平升高或正常的 NAFLD 组,以及肝酶水平正常的非 NAFLD 组。通过与全国性登记处的计算机化数据链接确定肝硬化和 HCC 的发生率。使用 Cox 比例风险模型估计 NAFLD 对肝硬化和 HCC 风险的危害比。
肝硬化和 HCC 的发病率如下升高:肝酶水平正常的非 NAFLD 组(n=66801;51%)、肝酶水平正常的 NAFLD 组(n=41461;32%)和肝酶水平升高的 NAFLD 组(n=21112;16%)。在肝酶水平升高的 NAFLD 组和肝酶水平正常的 NAFLD 组中,肝硬化的多变量调整危害比分别为 3.51(95%置信区间[CI]:2.36-5.22)和 0.73(95% CI:0.46-1.16),HCC 分别为 1.91(95% CI:1.08-3.38)和 0.57(95% CI:0.31-1.04),与非 NAFLD 组相比(趋势 P<.001)。在限制分析仅限于非肥胖个体(体重指数,<25 kg/m)和非肥胖个体且无糖尿病(P<.05)后,结果仍然一致。
肝酶水平升高的 NAFLD 患者肝硬化和 HCC 的风险显著增加,应进行监测。