Addiction Medicine Program, Oregon Health and Science University, Portland, OR, USA.
Oregon Health and Science University-Portland State University School of Public Health, Portland, OR, USA.
Addiction. 2022 Jul;117(7):1961-1971. doi: 10.1111/add.15836. Epub 2022 Mar 2.
Opioid agonist medications for treatment of opioid use disorder (OUD) can improve human immunodeficiency virus (HIV) outcomes and reduce opioid use. We tested whether outpatient antagonist treatment with naltrexone could achieve similar results.
Open-label, non-inferiority randomized trial.
Six US HIV primary care clinics.
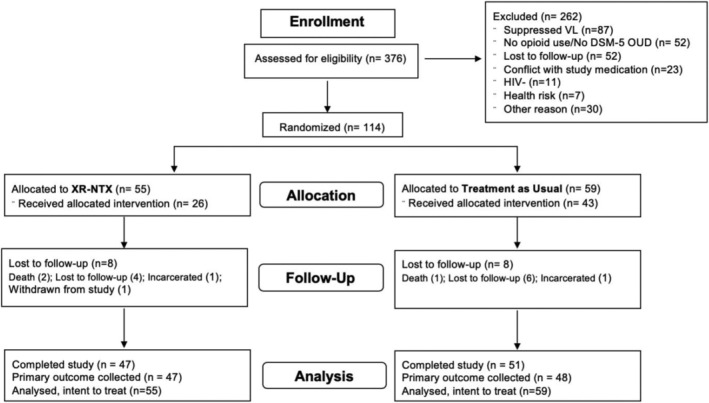
A total of 114 participants with untreated HIV and OUD (62% male; 56% black, 12% Hispanic; positive for fentanyl (62%), other opioids (47%) and cocaine (60%) at baseline). Enrollment halted early due to slow recruitment.
HIV clinic-based extended-release naltrexone (XR-NTX; n = 55) versus treatment as usual (TAU) with buprenorphine or methadone (TAU; n = 59).
Treatment group differences were compared for the primary outcome of viral suppression (HIV RNA ≤ 200 copies/ml) at 24 weeks and secondary outcomes included past 30-day use of opioids at 24 weeks.
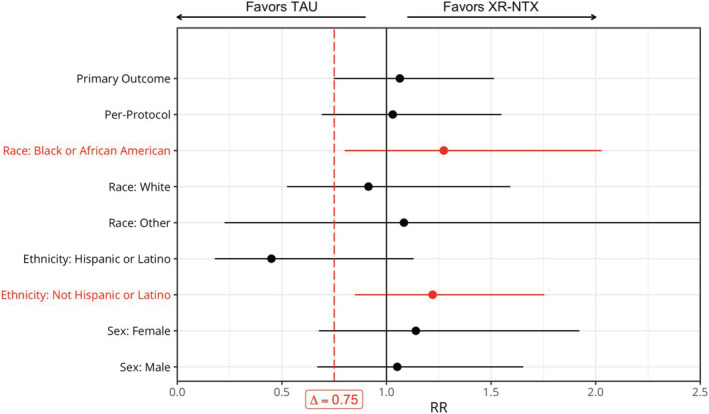
Fewer XR-NTX participants initiated medication compared with TAU participants (47 versus 73%). The primary outcome of viral suppression was comparable for XR-NTX (52.7%) and TAU (49.2%) [risk ratio (RR) = 1.064; 95% confidence interval (CI) = 0.748, 1.514] at 24 weeks. Non-inferiority could not be demonstrated, as the lower confidence limit of the RR did not exceed the pre-specified margin of 0.75 in intention-to-treat (ITT) analysis. The main secondary outcome of past 30-day opioid use was comparable for XR-NTX versus TAU (11.7 versus 14.8 days; mean difference = -3.1; 95% CI = -8.7, 1.1) in ITT analysis. Among those initiating medication, XR-NTX resulted in fewer days of opioid use compared with TAU in the past 30 days (6.0 versus 13.6, mean difference = -7.6; 95% CI = -13.8, -0.2).
A randomized controlled trial found supportive, but not conclusive, evidence that human immunodeficiency virus clinic-based extended-release naltrexone is not inferior to treatment as usual for facilitating human immunodeficiency virus viral suppression. Participants who initiated extended-release naltrexone used fewer opioids than those who received treatment as usual.
阿片类激动剂药物治疗阿片类药物使用障碍(OUD)可以改善人类免疫缺陷病毒(HIV)的结果并减少阿片类药物的使用。我们测试了纳曲酮的门诊拮抗剂治疗是否可以达到类似的效果。
开放标签,非劣效性随机试验。
六家美国 HIV 初级保健诊所。
共有 114 名未经治疗的 HIV 和 OUD 患者(62%为男性;56%为黑人,12%为西班牙裔;基线时芬太尼(62%)、其他阿片类药物(47%)和可卡因(60%)阳性)。由于招募缓慢,提前停止了试验。
HIV 诊所的延长释放纳曲酮(XR-NTX;n=55)与美沙酮或丁丙诺啡的常规治疗(TAU;n=59)。
比较病毒抑制(HIV RNA≤200 拷贝/ml)的主要结果在 24 周时以及次要结果包括过去 30 天内的阿片类药物使用在 24 周时。
与 TAU 参与者相比,接受 XR-NTX 的参与者开始药物治疗的人数较少(47 比 73%)。病毒抑制的主要结果在 XR-NTX(52.7%)和 TAU(49.2%)之间是可比的[风险比(RR)=1.064;95%置信区间(CI)=0.748, 1.514]在 24 周时。在 24 周时,非劣效性不能证明,因为 RR 的置信下限未超过预先指定的 0.75 界限,在意向治疗(ITT)分析中。XR-NTX 与 TAU 相比,过去 30 天内阿片类药物使用的主要次要结果是可比的(11.7 比 14.8 天;平均差异= -3.1;95%CI=-8.7, 1.1)在 ITT 分析中。在开始药物治疗的患者中,XR-NTX 在过去 30 天内的阿片类药物使用天数比 TAU 少(6.0 比 13.6,平均差异= -7.6;95%CI=-13.8, -0.2)。
一项随机对照试验提供了支持性但非结论性的证据,表明基于人类免疫缺陷病毒诊所的延长释放纳曲酮在促进人类免疫缺陷病毒病毒抑制方面并不劣于常规治疗。开始使用延长释放纳曲酮的参与者比接受常规治疗的参与者使用的阿片类药物更少。