Department of Pharmacology, University of Oxford, Oxford, UK.
Department of Chemistry, University of Oxford, Oxford, UK.
Liver Int. 2022 Jun;42(6):1344-1354. doi: 10.1111/liv.15192. Epub 2022 Feb 21.
BACKGROUND & AIMS: Primary sclerosing cholangitis (PSC) and IgG4-related sclerosing cholangitis (IgG4-SC) are chronic fibro-inflammatory immune-mediated hepatobiliary conditions that are challenging to distinguish in a clinical setting. Accurate non-invasive biomarkers for discriminating PSC and IgG4-SC are important to ensure a correct diagnosis, prompt therapy and adequate cancer surveillance.
We performed nuclear magnetic resonance (NMR)-based metabolomic profiling using serum samples collected prospectively from patients with PSC (n = 100), IgG4-SC (n = 23) and healthy controls (HC; n = 16).
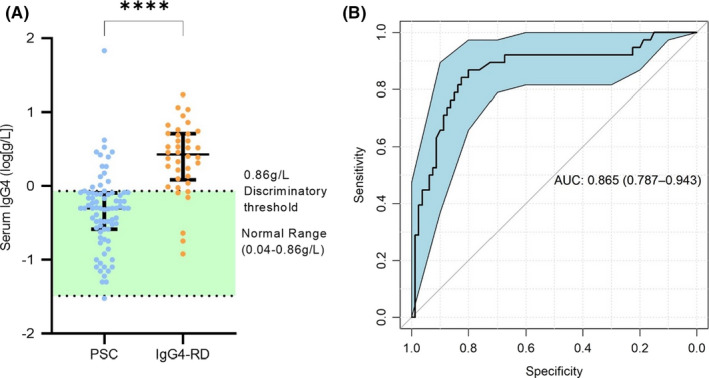
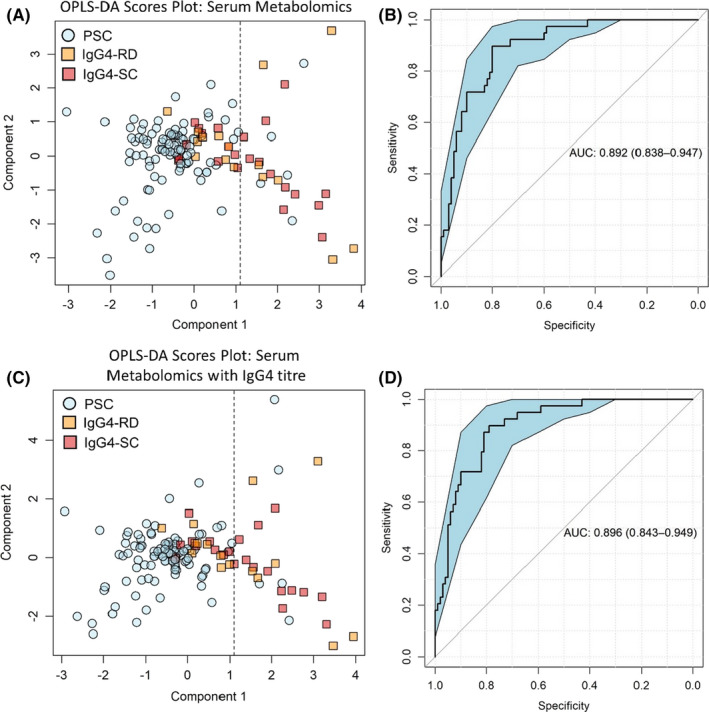
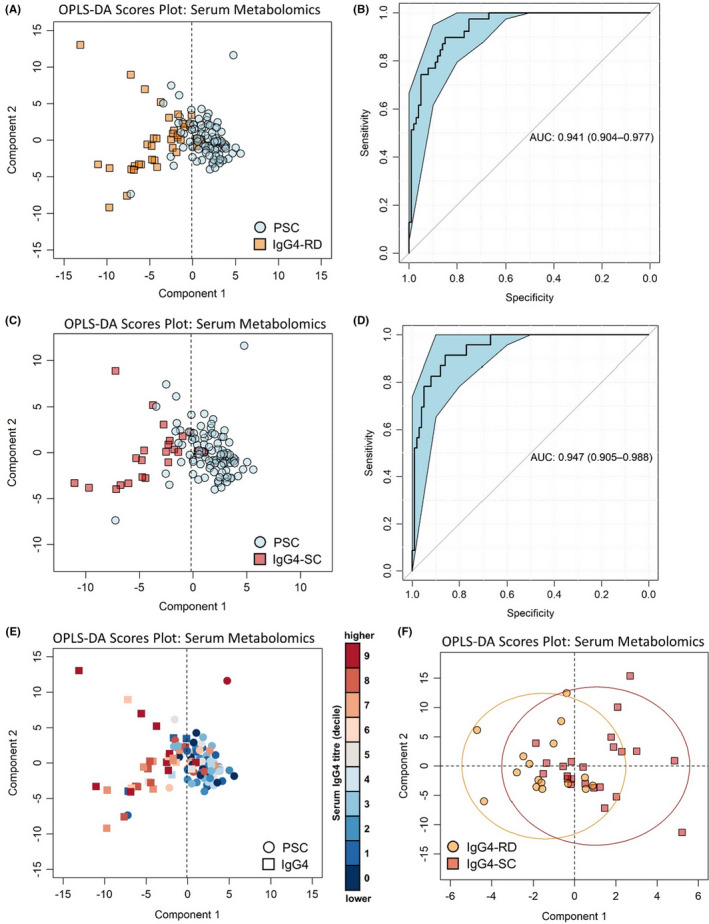
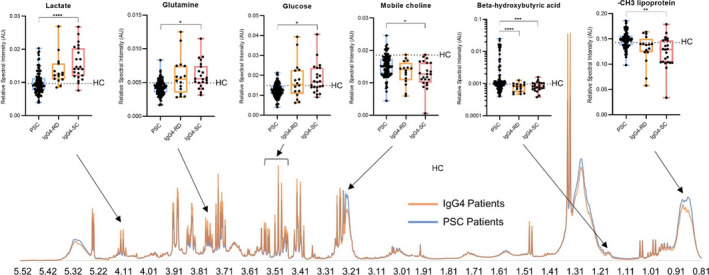
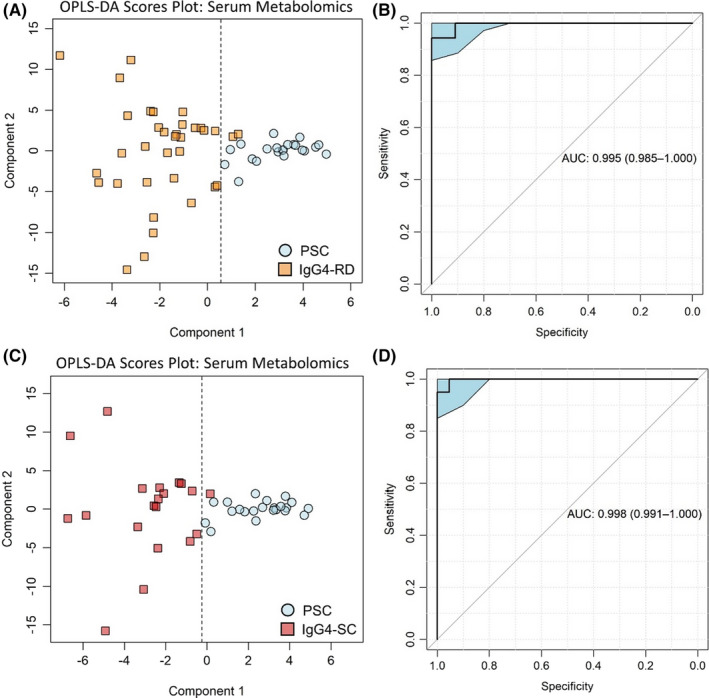
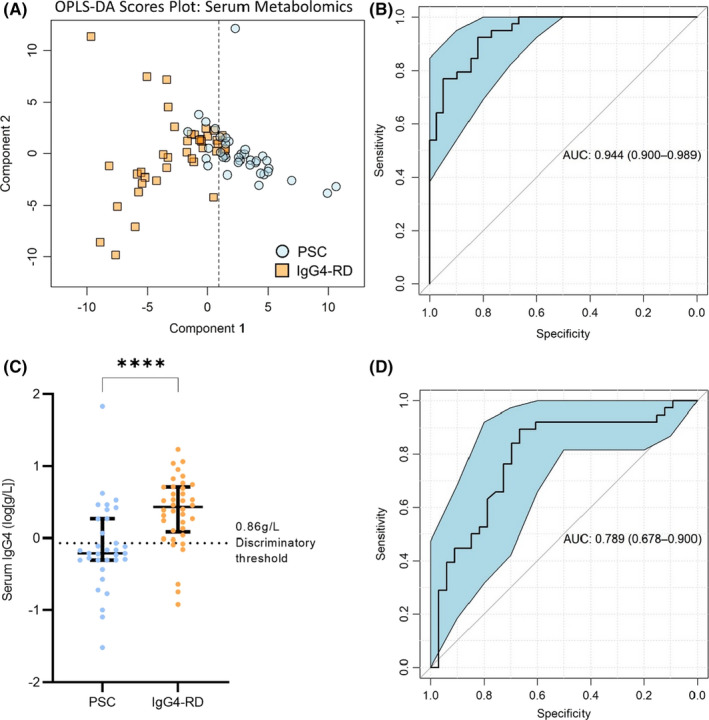
Multivariate analysis of the serum metabolome discriminated PSC from IgG4-SC with greater accuracy (AUC 0.95 [95%CI 0.90-0.98]) than IgG4 titre (AUC 0.87 [95%CI 0.79-0.94]). When inflammatory bowel disease (IBD) was excluded as a comorbid condition (IgG4-SC n = 20, PSC n = 22), the diagnostic AUC increased to 1.0, suggesting that the metabolome differences identified are not a result of the increased prevalence of IBD in PSC relative to IgG4-SC patients. Serum lactate (p < .0001), glucose (p < .01) and glutamine (p < .01) metabolites were increased in IgG4-related disease (IgG4-RD) and IgG4-SC individuals compared to PSC, whereas mobile choline (p < .05), 3-hydroxybutyric acid (p < .01) and -CH lipoprotein resonances (p < .01) were decreased.
Taken together, serum metabolomic profiling has the potential to be incorporated as a diagnostic criterion, independent of IgG4 titre, to improve the diagnosis of IgG4-RD and help distinguish IgG4-SC from PSC.
原发性硬化性胆管炎(PSC)和 IgG4 相关硬化性胆管炎(IgG4-SC)是慢性纤维炎症性免疫介导的肝胆疾病,在临床环境中难以区分。准确的非侵入性生物标志物对于区分 PSC 和 IgG4-SC 非常重要,可以确保正确的诊断、及时的治疗和充分的癌症监测。
我们使用前瞻性收集的 PSC(n=100)、IgG4-SC(n=23)和健康对照者(HC;n=16)的血清样本进行基于核磁共振(NMR)的代谢组学分析。
对血清代谢组的多变量分析能够更准确地区分 PSC 和 IgG4-SC(AUC 0.95 [95%CI 0.90-0.98]),优于 IgG4 滴度(AUC 0.87 [95%CI 0.79-0.94])。当排除炎症性肠病(IBD)作为合并症(IgG4-SC n=20,PSC n=22)时,诊断 AUC 增加到 1.0,表明所鉴定的代谢组差异不是由于 PSC 患者中 IBD 的患病率高于 IgG4-SC 患者所致。与 PSC 相比,IgG4 相关疾病(IgG4-RD)和 IgG4-SC 个体的血清乳酸盐(p<0.0001)、葡萄糖(p<0.01)和谷氨酰胺(p<0.01)代谢物升高,而移动胆碱(p<0.05)、3-羟基丁酸(p<0.01)和-CH 脂蛋白共振(p<0.01)降低。
综上所述,血清代谢组学分析有可能被纳入诊断标准,独立于 IgG4 滴度,以改善 IgG4-RD 的诊断,并有助于区分 IgG4-SC 和 PSC。