Princess Máxima Center for Pediatric Oncology, Utrecht, The Netherlands.
University Medical Center Utrecht, Utrecht, The Netherlands.
Blood Adv. 2022 Apr 12;6(7):1969-1976. doi: 10.1182/bloodadvances.2021006700.
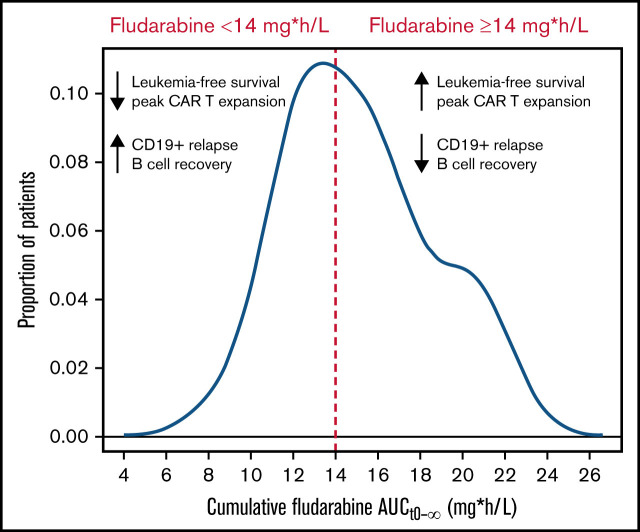
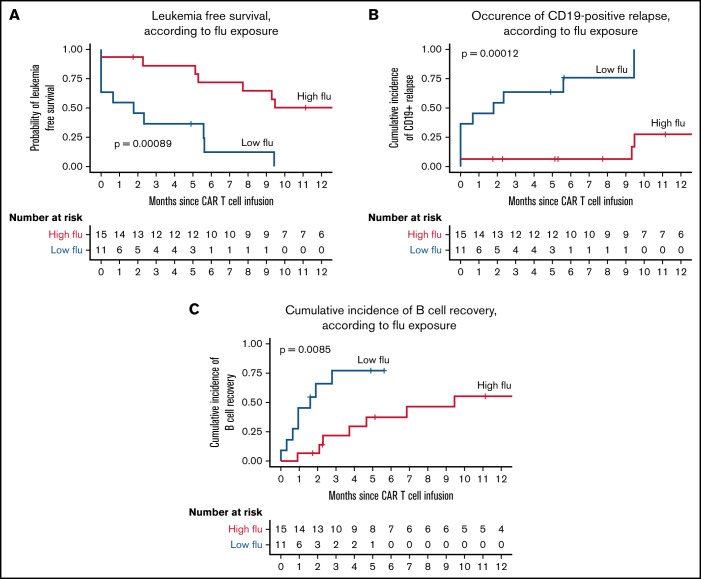
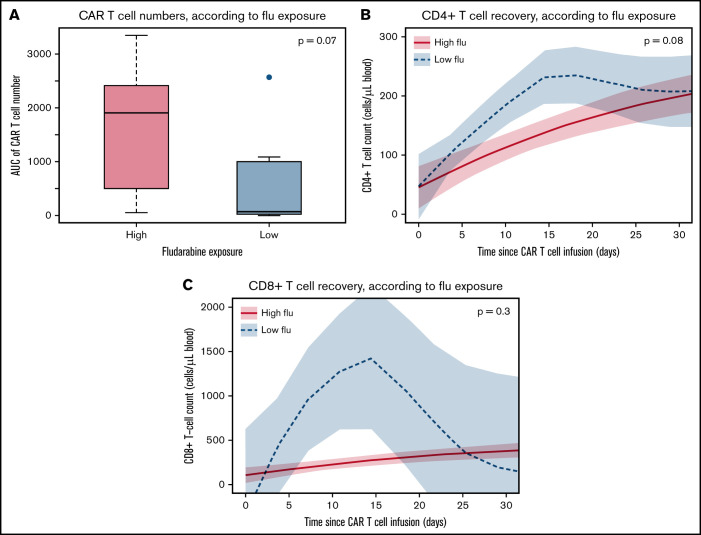
The addition of fludarabine to cyclophosphamide as a lymphodepleting regimen prior to CD19 chimeric antigen receptor (CAR) T-cell therapy significantly improved outcomes in patients with relapsed/refractory (r/r) B-cell acute lymphoblastic leukemia (B-ALL). Fludarabine exposure, previously shown to be highly variable when dosing is based on body surface area (BSA), is a predictor for survival in allogeneic hematopoietic cell transplantation (allo-HCT). Hence, we hypothesized that an optimal exposure of fludarabine might be of clinical importance in CD19 CAR T-cell treatment. We examined the effect of cumulative fludarabine exposure during lymphodepletion, defined as concentration-time curve (AUC), on clinical outcome and lymphocyte kinetics. A retrospective analysis was conducted with data from 26 patients receiving tisagenlecleucel for r/r B-ALL. Exposure of fludarabine was shown to be a predictor for leukemia-free survival (LFS), B-cell aplasia, and CD19-positive relapse following CAR T-cell infusion. Minimal event probability was observed at a cumulative fludarabine AUCT0-∞ ≥14 mgh/L, and underexposure was defined as an AUCT0-∞ <14 mgh/L. In the underexposed group, the median LFS was 1.8 months, and the occurrence of CD19-positive relapse within 1 year was 100%, which was higher compared with the group with an AUCT0-∞ ≥14 mg*h/L (12.9 months; P < .001; and 27.4%; P = .0001, respectively). Furthermore, the duration of B-cell aplasia within 6 months was shorter in the underexposed group (77.3% vs 37.3%; P = .009). These results suggest that optimizing fludarabine exposure may have a relevant impact on LFS following CAR T-cell therapy, which needs to be validated in a prospective clinical trial.
在接受 CD19 嵌合抗原受体(CAR)T 细胞治疗之前,用氟达拉滨联合环磷酰胺作为淋巴清除方案可显著改善复发/难治性(r/r)B 细胞急性淋巴细胞白血病(B-ALL)患者的结局。氟达拉滨的暴露量先前已被证明在基于体表面积(BSA)给药时高度可变,是异基因造血细胞移植(allo-HCT)中生存的预测因子。因此,我们假设氟达拉滨的最佳暴露量在 CD19 CAR T 细胞治疗中可能具有临床意义。我们研究了淋巴清除期间累积氟达拉滨暴露量(定义为浓度-时间曲线下面积[AUC])对临床结局和淋巴细胞动力学的影响。对 26 例接受 tisagenlecleucel 治疗 r/r B-ALL 的患者进行了回顾性分析。氟达拉滨的暴露量被证明是无白血病生存(LFS)、B 细胞再生障碍和 CAR T 细胞输注后 CD19 阳性复发的预测因子。在累积氟达拉滨 AUC0-∞≥14mgh/L 时观察到最小事件概率,而暴露不足定义为 AUC0-∞<14mgh/L。在暴露不足组中,中位 LFS 为 1.8 个月,1 年内 CD19 阳性复发的发生率为 100%,高于 AUC0-∞≥14mg*h/L 组(12.9 个月;P<0.001;和 27.4%;P=0.0001,分别)。此外,暴露不足组中 6 个月内 B 细胞再生障碍的持续时间更短(77.3%对 37.3%;P=0.009)。这些结果表明,优化氟达拉滨暴露量可能对 CAR T 细胞治疗后 LFS 产生相关影响,这需要在前瞻性临床试验中得到验证。