Bundy Joshua D, Rahman Mahboob, Matsushita Kunihiro, Jaeger Byron C, Cohen Jordana B, Chen Jing, Deo Rajat, Dobre Mirela A, Feldman Harold I, Flack John, Kallem Radhakrishna R, Lash James P, Seliger Stephen, Shafi Tariq, Weiner Shoshana J, Wolf Myles, Yang Wei, Allen Norrina B, Bansal Nisha, He Jiang
Department of Epidemiology, Tulane University School of Public Health and Tropical Medicine, New Orleans, Louisiana.
Tulane University Translational Science Institute, New Orleans, Louisiana.
J Am Soc Nephrol. 2022 Mar;33(3):601-611. doi: 10.1681/ASN.2021060747. Epub 2022 Feb 10.
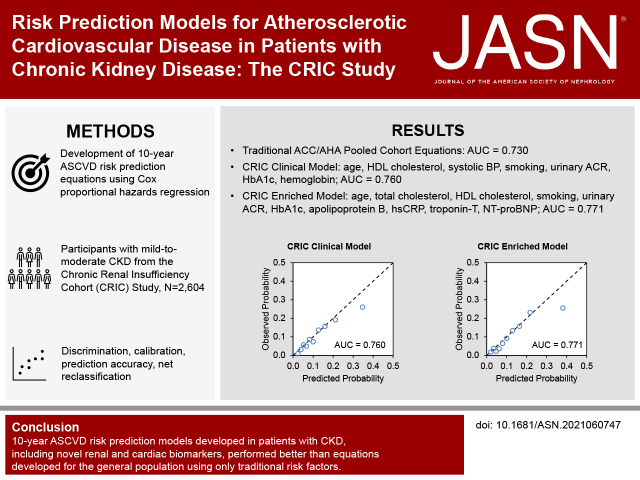
Individuals with CKD may be at high risk for atherosclerotic cardiovascular disease (ASCVD). However, there are no ASCVD risk prediction models developed in CKD populations to inform clinical care and prevention.
We developed and validated 10-year ASCVD risk prediction models in patients with CKD that included participants without self-reported cardiovascular disease from the Chronic Renal Insufficiency Cohort (CRIC) study. ASCVD was defined as the first occurrence of adjudicated fatal and nonfatal stroke or myocardial infarction. Our models used clinically available variables and novel biomarkers. Model performance was evaluated based on discrimination, calibration, and net reclassification improvement.
Of 2604 participants (mean age 55.8 years; 52.0% male) included in the analyses, 252 had incident ASCVD within 10 years of baseline. Compared with the American College of Cardiology/American Heart Association pooled cohort equations (area under the receiver operating characteristic curve [AUC]=0.730), a model with coefficients estimated within the CRIC sample had higher discrimination (=0.03), achieving an AUC of 0.736 (95% confidence interval [CI], 0.649 to 0.826). The CRIC model developed using clinically available variables had an AUC of 0.760 (95% CI, 0.678 to 0.851). The CRIC biomarker-enriched model had an AUC of 0.771 (95% CI, 0.674 to 0.853), which was significantly higher than the clinical model (=0.001). Both the clinical and biomarker-enriched models were well-calibrated and improved reclassification of nonevents compared with the pooled cohort equations (6.6%; 95% CI, 3.7% to 9.6% and 10.0%; 95% CI, 6.8% to 13.3%, respectively).
The 10-year ASCVD risk prediction models developed in patients with CKD, including novel kidney and cardiac biomarkers, performed better than equations developed for the general population using only traditional risk factors.
慢性肾脏病(CKD)患者可能面临动脉粥样硬化性心血管疾病(ASCVD)的高风险。然而,目前尚无专门为CKD人群开发的ASCVD风险预测模型来指导临床护理和预防工作。
我们在CKD患者中开发并验证了10年ASCVD风险预测模型,纳入了慢性肾功能不全队列(CRIC)研究中无自我报告心血管疾病的参与者。ASCVD定义为首次发生经判定的致命性和非致命性中风或心肌梗死。我们的模型使用了临床可用变量和新型生物标志物。基于辨别力、校准度和净重新分类改善情况对模型性能进行评估。
分析纳入的2604名参与者(平均年龄55.8岁;52.0%为男性)中,252人在基线后10年内发生了ASCVD事件。与美国心脏病学会/美国心脏协会合并队列方程(受试者工作特征曲线下面积[AUC]=0.730)相比,在CRIC样本中估计系数的模型具有更高的辨别力(=0.03),AUC为0.736(95%置信区间[CI],0.649至0.826)。使用临床可用变量开发的CRIC模型AUC为0.760(95%CI,0.678至0.851)。富含生物标志物的CRIC模型AUC为0.771(95%CI,0.674至0.853),显著高于临床模型(=0.001)。与合并队列方程相比,临床模型和富含生物标志物的模型校准良好,且改善了非事件的重新分类(分别为6.6%;95%CI,3.7%至9.6%和10.0%;95%CI,6.8%至13.3%)。
在CKD患者中开发的10年ASCVD风险预测模型,包括新型肾脏和心脏生物标志物,比仅使用传统风险因素为一般人群开发的方程表现更好。