Department of Cardiology, Radboud University Medical Center, Geert Grooteplein 10, 6525 GA, Nijmegen, The Netherlands.
Department of Radiology, University Medical Center Utrecht, Utrecht, The Netherlands.
Int J Cardiovasc Imaging. 2022 Aug;38(8):1699-1710. doi: 10.1007/s10554-022-02555-6. Epub 2022 Feb 21.
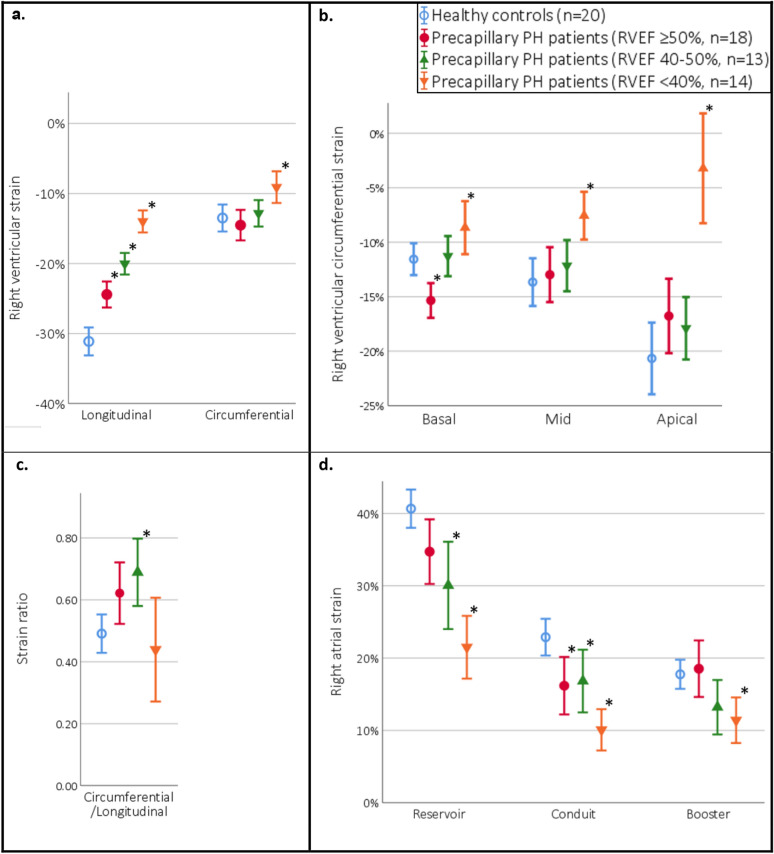
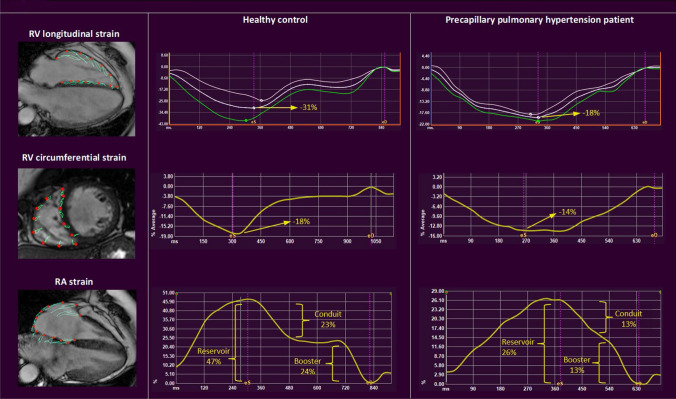
Right ventricular (RV) ejection fraction (EF) by cardiac magnetic resonance (CMR) correlates to outcome in precapillary pulmonary hypertension (pPH) patients, but is insensitive to early changes. Strain might provide incremental information. In this study, we compare right atrial (RA) and RV strain in pPH patients to healthy controls, and evaluate the prognostic value of strain in pPH. In this cross-sectional study, 45 pPH patients and 20 healthy controls underwent CMR, and feature-tracking derived RA and RV strain were evaluated. pPH patients had impaired RA reservoir and conduit strain, and RV longitudinal strain (LS), compared to healthy controls. In pPH patients with preserved RVEF (≥ 50%, n = 18), RA reservoir (35% ± 9 vs. 41% ± 6, p = 0.02) and conduit strain (16% ± 8 vs. 23% ± 5, p = 0.004), and RV-LS (-25% ± 4 vs. -31% ± 4, p < 0.001) remained impaired, compared to healthy controls. The association of strain with the primary endpoint (combination of all-cause death, lung transplantation, and heart failure hospitalization) was evaluated using a multivariable Cox regression model. RV-LS (HR 1.18, 95%-CI 1.04-1.34, p = 0.01) and RA strain (reservoir: HR 0.87, 95%-CI 0.80-0.94, p = 0.001; conduit: HR 0.85, 95%-CI 0.75-0.97, p = 0.02, booster: HR 0.81, 95%-CI 0.71-0.92, p = 0.001) were independent predictors of outcome, beyond clinical and imaging features. In conclusion, pPH patients have impaired RA strain and RV-LS, even when RVEF is preserved. In addition, RA strain and RV-LS were independent predictors of adverse prognosis. These results emphasize the incremental value of RA and RV strain analyses, to detect alterations in RV function, even before RVEF declines.
右心室(RV)射血分数(EF)通过心脏磁共振(CMR)与毛细血管前肺动脉高压(pPH)患者的预后相关,但对早期变化不敏感。应变可能提供额外的信息。在这项研究中,我们比较了 pPH 患者和健康对照组的右心房(RA)和 RV 应变,并评估了应变在 pPH 中的预后价值。在这项横断面研究中,45 名 pPH 患者和 20 名健康对照组接受了 CMR,评估了特征跟踪衍生的 RA 和 RV 应变。与健康对照组相比,pPH 患者的 RA 储备和输送应变以及 RV 纵向应变(LS)受损。在 RVEF(≥50%,n=18)保留的 pPH 患者中,RA 储备(35%±9% vs. 41%±6%,p=0.02)和输送应变(16%±8% vs. 23%±5%,p=0.004)以及 RV-LS(-25%±4% vs. -31%±4%,p<0.001)仍然受损。使用多变量 Cox 回归模型评估应变与主要终点(全因死亡、肺移植和心力衰竭住院的组合)的相关性。RV-LS(HR 1.18,95%-CI 1.04-1.34,p=0.01)和 RA 应变(储备:HR 0.87,95%-CI 0.80-0.94,p=0.001;输送:HR 0.85,95%-CI 0.75-0.97,p=0.02,升压:HR 0.81,95%-CI 0.71-0.92,p=0.001)是预后的独立预测因素,超出了临床和影像学特征。总之,即使 RVEF 保留,pPH 患者也存在 RA 应变和 RV-LS 受损。此外,RA 应变和 RV-LS 是不良预后的独立预测因素。这些结果强调了 RA 和 RV 应变分析的增量价值,即使在 RVEF 下降之前,也可以检测 RV 功能的变化。