Nekoukar Zahra, Ala Shahram, Moradi Siavash, Hill Andrew, Davoudi Badabi Ali Reza, Alikhani Ahmad, Alian Shahriar, Moghimi Minoo, Shabani Amir Mohammad, Abbaspour Kasgari Hamideh
Department of Clinical Pharmacy, School of Pharmacy, Mazandaran University of Medical Sciences, Sari, Iran.
Education Development Center, Mazandaran University of Medical Sciences, Sari, Iran.
Iran J Pharm Res. 2021 Fall;20(4):278-288. doi: 10.22037/ijpr.2021.115157.15243.
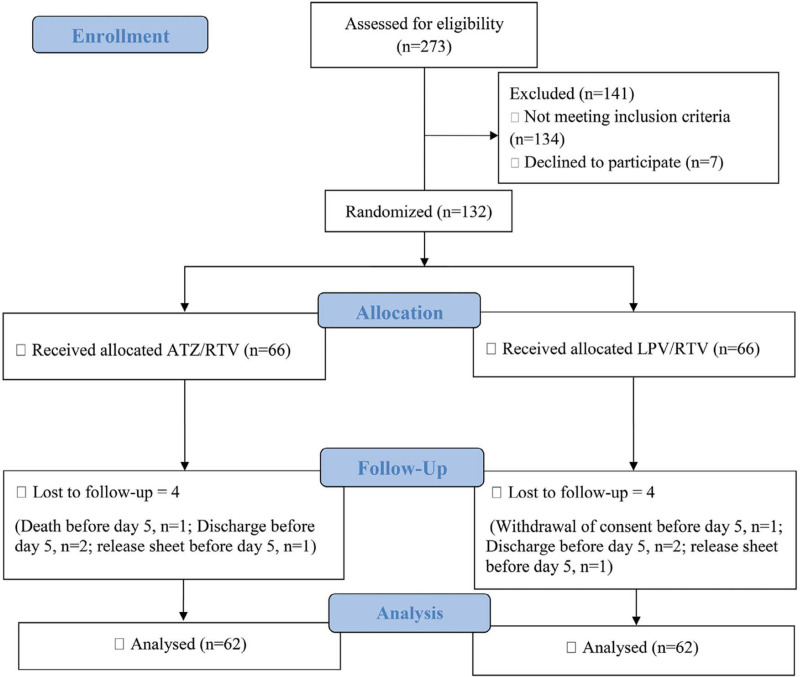
This was a randomized, double-blind clinical trial to compare the efficacy and safety of Atazanavir/Ritonavir (ATZ/RTV) with Lopinavir/Ritonavir (LPV/RTV) in moderate Coronavirus disease 2019 (COVID-19). Participants were randomly assigned to receive a single dose of hydroxychloroquine (HCQ) plus ATZ/RTV or LPV/RTV for a minimum of 5 to a maximum of 10 days. The primary outcomes were the reduced length of hospital stay and clinical recovery within 10 days from starting the intervention. The rate of intensive care unit (ICU) admission, intubation, and mortality, the lengths of ICU stay and being intubated, recovery within 14 days, and the frequency of adverse reactions were considered as secondary outcomes. Among 132 enrolled patients, 62 cases in each arm were analyzed at the end of the intervention. Fifty-one (82.3%) cases in the ATZ/RTV arm versus 41 (66.1%) in the LPV/RTV arm were discharged within 10 days ( 0.06). The median number of the intervention days was 6 (IQR: 5-8) in ATZ/RTV arm versus 7 (IQR: 6-9) in LPV/RTV arm ( 0.01). The rate and length of ICU admission and intubation ( ≥ 0.99), rate of mortality ( 0.49), and recovery within 14 days ( 0.09) were not statistically different between groups. The most reported adverse reactions were nausea and vomiting that all cases were in the LPV/RTV arm ( = 0.006). ATZ/RTV is better tolerated in comparison with LPV/RTV; however, it did not show more efficacy than LPV/RTV in clinical outcomes of COVID-19 in this study.
这是一项随机、双盲临床试验,旨在比较阿扎那韦/利托那韦(ATZ/RTV)与洛匹那韦/利托那韦(LPV/RTV)治疗中度2019冠状病毒病(COVID-19)的疗效和安全性。参与者被随机分配接受单剂量羟氯喹(HCQ)加ATZ/RTV或LPV/RTV,疗程至少5天、最长10天。主要结局为干预开始后10天内住院时间缩短和临床康复。重症监护病房(ICU)入院率、插管率和死亡率、ICU住院时间和插管时间、14天内康复情况以及不良反应发生率被视为次要结局。在132名入组患者中,干预结束时对每组62例进行分析。ATZ/RTV组51例(82.3%)患者与LPV/RTV组41例(66.1%)患者在10天内出院( = 0.06)。ATZ/RTV组干预天数中位数为6天(四分位间距:5 - 8天),而LPV/RTV组为7天(四分位间距:6 - 9天)( = 0.01)。两组间ICU入院率和插管率及时间( ≥ 0.99)、死亡率( 0.49)和14天内康复情况( 0.09)无统计学差异。报告最多的不良反应是恶心和呕吐,所有病例均在LPV/RTV组( = 0.006)。与LPV/RTV相比,ATZ/RTV耐受性更好;然而,在本研究中,ATZ/RTV在COVID-19临床结局方面未显示出比LPV/RTV更有效。