Department of Surgery, Amsterdam University Medical Centres (UMC), University of Amsterdam, Cancer Centre Amsterdam, Meibergdreef 9, Amsterdam, the Netherlands.
Division of Digestive Surgery, University Hospitals of Geneva, 1205, Geneva, Switzerland.
Surg Endosc. 2022 Oct;36(10):7369-7375. doi: 10.1007/s00464-022-09136-7. Epub 2022 Feb 23.
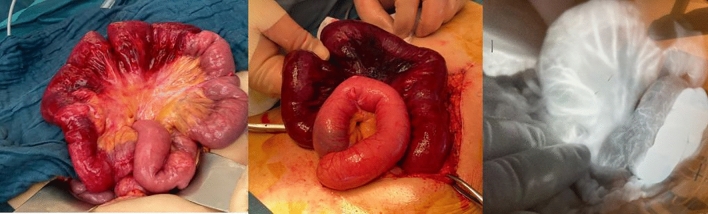
Assessing bowel viability can be challenging during acute surgical procedures, especially regarding mesenteric ischaemia. Intraoperative fluorescence angiography (FA) may be a valuable tool for the surgeon to determine whether bowel resection is necessary and to define the most appropriate resection margins. The aim of this study is to report on FA use in the acute setting and to judge its impact on intraoperative decision making.
This is a multi-centre, retrospective case series of patients undergoing emergency abdominal surgery between February 2016 and 2021 in three general/colorectal units where intraoperative FA was performed to assess bowel viability. Primary endpoint was change of management after the FA assessment.
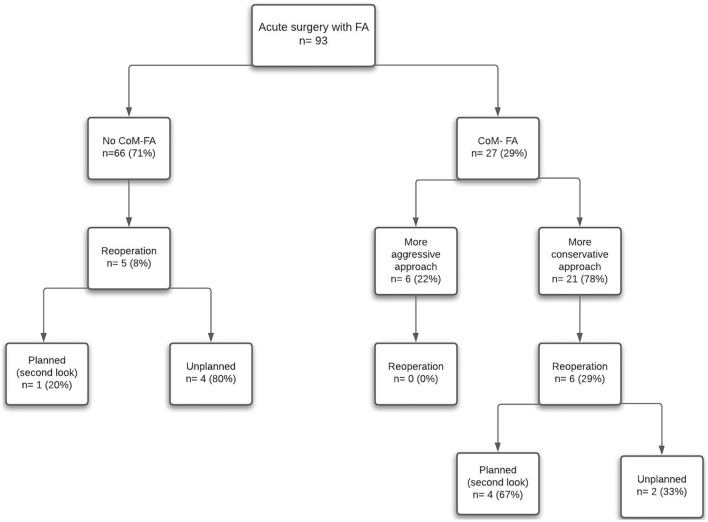
A total of 93 patients (50 males, 66.6 ± 19.2 years, ASA score ≥ III in 85%) were identified and studied. Initial surgical approach was laparotomy in 66 (71%) patients and laparoscopy in 27 (29% and seven, 26% conversions). The most common aetiologies were mesenteric ischaemia (n = 42, 45%) and adhesional/herniae-related strangulation (n = 41, 44%). In 50 patients a bowel resection was performed. Overall rates of anastomosis after resection, reoperation and 30-day mortality were 48% (n = 24/50, one leak), 12% and 18%, respectively. FA changed management in 27 (29%) patients. In four patients (4% overall), resection was avoided and in 21 (23%) extra bowel length was preserved (median 50 cm of bowel saved, IQR 28-98) although three patients developed further ischaemia. FA prompted extended resection (median of 20 cm, IQR 10-50 extra bowel) in six (6%) patients.
Intraoperative use of FA impacts surgical decisions regarding bowel resection for intestinal ischaemia, potentially enabling bowel preservation in approximately one out of four patients. Prospective studies are needed to optimize the best use of this technology for this indication and to determine standards for the interpretation of FA images and the potential subsequent need for second-look surgeries.
在急性外科手术中,评估肠活力可能具有挑战性,特别是涉及肠系膜缺血的情况。术中荧光血管造影(FA)可能是外科医生确定是否需要肠切除术并定义最合适的切除范围的有用工具。本研究的目的是报告 FA 在急性情况下的应用,并判断其对术中决策的影响。
这是一项多中心、回顾性病例系列研究,纳入了 2016 年 2 月至 2021 年期间在三个普通/结直肠外科单位接受紧急腹部手术的患者,这些单位在术中进行 FA 评估以评估肠活力。主要终点是 FA 评估后管理的变化。
共确定并研究了 93 名患者(50 名男性,66.6±19.2 岁,ASA 评分≥III 级的 85%)。初始手术方法为剖腹手术 66 例(71%)和腹腔镜手术 27 例(29%,其中 7 例为 26%的中转)。最常见的病因是肠系膜缺血(n=42,45%)和粘连/疝相关绞窄(n=41,44%)。50 例患者行肠切除术。总体切除后吻合、再次手术和 30 天死亡率分别为 48%(n=24/50,1 例漏)、12%和 18%。FA 改变了 27 例(29%)患者的治疗方案。4 例(总体 4%)避免了切除,21 例(23%)保留了额外的肠段(中位保留肠段 50cm,IQR 28-98),尽管其中 3 例发生进一步缺血。FA 促使 6 例(6%)患者进行了扩大切除(中位切除 20cm,IQR 10-50cm 额外肠段)。
术中使用 FA 影响了肠缺血患者的肠切除术决策,可能使大约四分之一的患者能够保留肠段。需要前瞻性研究来优化该技术在该适应证中的最佳应用,并确定 FA 图像解释的标准以及潜在的后续二次手术的需求。