Vecsey-Nagy Milán, Szilveszter Bálint, Kolossváry Márton, Boussoussou Melinda, Vattay Borbála, Merkely Béla, Maurovich-Horvat Pál, Radovits Tamás, Nemcsik János
MTA-SE Cardiovascular Imaging Research Group, Heart and Vascular Center, Semmelweis University, 1122 Budapest, Hungary.
Cardiology Department, Heart and Vascular Center, Semmelweis University, 1122 Budapest, Hungary.
J Clin Med. 2022 Feb 19;11(4):1111. doi: 10.3390/jcm11041111.
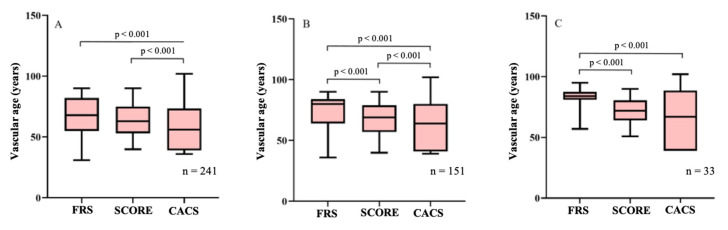
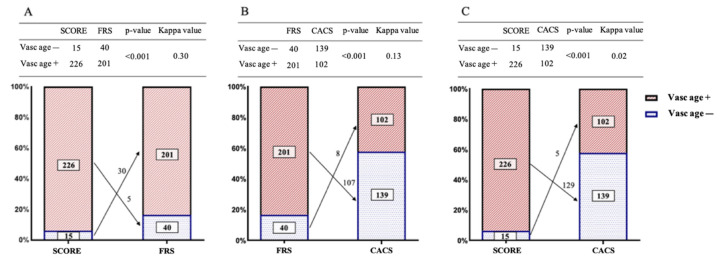
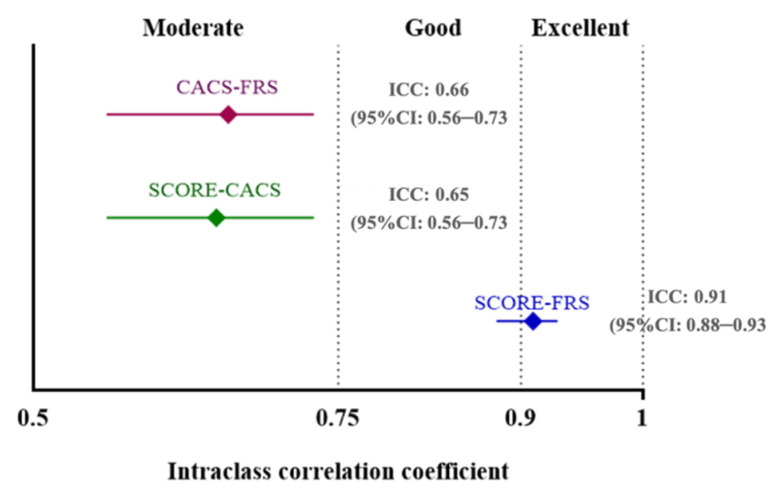
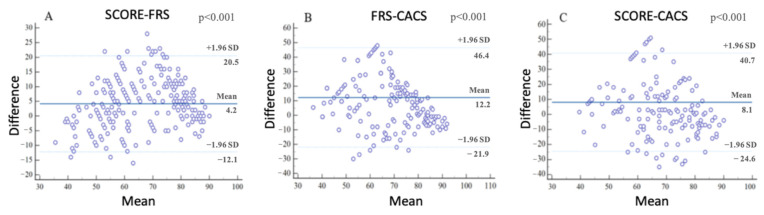
Vascular age can be derived from cardiovascular (CV) risk scores such as the Framingham Risk Score (FRS) and the Systematic Coronary Risk Evaluation (SCORE). Recently, coronary artery calcium score (CACS) was proposed as a means of assessing arterial age. We aimed to compare these approaches for the assessment of vascular age. FRS-, SCORE-, and CACS-based vascular ages of 241 consecutive Caucasian patients undergoing coronary CT angiography were defined according to previously published methods. Vascular ages based on FRS, SCORE, and CACS were 68.0 (IQR: 55.0-82.0), 63.0 (IQR: 53.0-75.0), and 47.1 (IQR: 39.1-72.3) years, respectively, ( < 0.001). FRS- and SCORE-based biological age showed strong correlation [ICC: 0.91 (95%CI: 0.88-0.93)], while CACS-based vascular age moderately correlated with FRS- and SCORE-based vascular age [ICC: 0.66 (95%CI: 0.56-0.73) and ICC: 0.65 (95%CI: 0.56-0.73), respectively, both < 0.001)]. Based on FRS, SCORE, and CACS, 83.4%, 93.8%, and 42.3% of the subjects had higher vascular age than their documented chronological age (FRS+, SCORE+, CACS+), and 53.2% of the FRS+ (107/201) and 57.1% of the SCORE+ (129/226) groups were classified as CACS-. Traditional risk equations demonstrate a tendency of overestimating vascular age in low- to intermediate-risk patients compared to CACS. Prospective studies are warranted to further evaluate the contribution of different vascular age calculations to CV preventive strategies.
血管年龄可从心血管(CV)风险评分得出,如弗雷明汉风险评分(FRS)和系统性冠状动脉风险评估(SCORE)。最近,冠状动脉钙化评分(CACS)被提议作为评估动脉年龄的一种方法。我们旨在比较这些评估血管年龄的方法。根据先前发表的方法,对241例连续接受冠状动脉CT血管造影的白种人患者基于FRS、SCORE和CACS的血管年龄进行了定义。基于FRS、SCORE和CACS的血管年龄分别为68.0(四分位间距:55.0 - 82.0)岁、63.0(四分位间距:53.0 - 75.0)岁和47.1(四分位间距:39.1 - 72.3)岁(<0.001)。基于FRS和SCORE的生物学年龄显示出强相关性[组内相关系数(ICC):0.91(95%置信区间:0.88 - 0.93)],而基于CACS的血管年龄与基于FRS和SCORE的血管年龄呈中度相关[ICC分别为0.66(95%置信区间:0.56 - 0.73)和0.65(95%置信区间:0.56 - 0.73),均<0.001]。基于FRS、SCORE和CACS,分别有83.4%、93.8%和42.3%的受试者血管年龄高于其记录的实际年龄(FRS+、SCORE+、CACS+),FRS+组(107/201)的53.2%和SCORE+组(129/226)的57.1%被归类为CACS-。与CACS相比,传统风险方程显示出在低至中度风险患者中高估血管年龄的趋势。有必要进行前瞻性研究以进一步评估不同血管年龄计算方法对心血管预防策略的贡献。