Department of Infectious Diseases, Alfred Hospital and Central Clinical School, Monash University, Melbourne, Victoria, Australia.
University of Queensland Centre for Clinical Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia.
J Antimicrob Chemother. 2022 Apr 27;77(5):1324-1333. doi: 10.1093/jac/dkac045.
The use of oral fosfomycin for urinary tract infections (UTIs) caused by non-Escherichia coli uropathogens is uncertain, including Klebsiella pneumoniae, the second most common uropathogen.
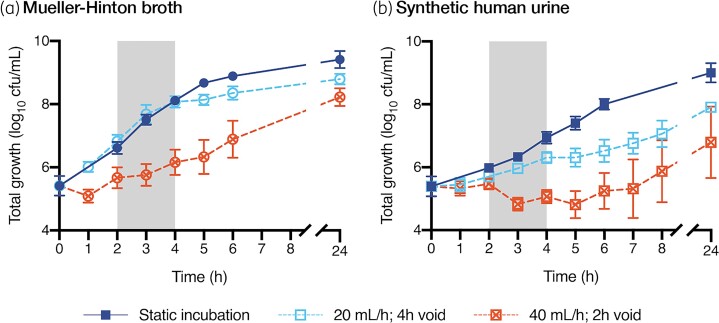
A multicompartment bladder infection in vitro model was used with standard media and synthetic human urine (SHU) to simulate urinary fosfomycin exposure after a single 3 g oral dose (fAUC0-72 16884 mg·h/L, t½ 5.5 h) against 15 K. pneumoniae isolates including ATCC 13883 (MIC 2 to >1024 mg/L) with a constant media inflow (20 mL/h) and 4-hourly voiding of each bladder. The impact of the media (CAMHB + G6P versus SHU) on fosfomycin MIC measurements, drug-free growth kinetics and regrowth after fosfomycin administration was assessed. A low and high starting inoculum (5.5 versus 7.5 log10 cfu/mL) was assessed in the bladder infection model.
Compared with CAMHB, isolates in SHU had a slower growth rate doubling time (37.7 versus 24.1 min) and reduced growth capacity (9.0 ± 0.3 versus 9.4 ± 0.3 log10 cfu/mL), which was further restricted with increased inflow rate (40 mL/h) and more frequent voids (2-hourly). Regrowth was commonly observed in both media with emergence of fosfomycin resistance promoted by a high starting inoculum in CAMHB (MIC rise to ≥1024 mg/L in 13/14 isolates). Resistance was rarely detected in SHU, even with a high starting inoculum (MIC rise to ≥1024 mg/L in 2/14 isolates).
Simulated in an in vitro UTI model, the regrowth of K. pneumoniae urinary isolates was inadequately suppressed following oral fosfomycin therapy. Efficacy was further reduced by a high starting inoculum.
对于非大肠埃希菌尿路病原体引起的尿路感染(UTI),使用口服磷霉素的效果尚不确定,包括肺炎克雷伯菌,这是第二常见的尿路病原体。
采用多室膀胱感染体外模型,使用标准培养基和合成人尿(SHU)模拟单次口服 3 克磷霉素后的尿液暴露情况(fAUC0-72 为 16884 毫克·小时/升,t½ 为 5.5 小时),针对 15 株肺炎克雷伯菌分离株,包括 ATCC 13883(MIC2 至>1024 毫克/升),培养基以恒定流速(20 毫升/小时)流入,每 4 小时排空膀胱。评估培养基(CAMHB+G6P 与 SHU)对磷霉素 MIC 测量、无药生长动力学和磷霉素给药后的再生长的影响。在膀胱感染模型中评估低和高起始接种量(5.5 对数 10 cfu/ml 与 7.5 对数 10 cfu/ml)。
与 CAMHB 相比,SHU 中的分离株生长倍增时间较慢(37.7 分钟与 24.1 分钟),生长能力降低(9.0 ±0.3 对数 10 cfu/ml 与 9.4 ±0.3 对数 10 cfu/ml),随着流入率增加(40 毫升/小时)和排空频率增加(每 2 小时排空一次),这种情况进一步受到限制。两种培养基中均常观察到再生长,高起始接种量在 CAMHB 中促进了磷霉素耐药性的出现(14 株分离株中有 13 株 MIC 上升至≥1024 毫克/升)。在 SHU 中耐药性很少被检测到,即使起始接种量较高(14 株分离株中有 2 株 MIC 上升至≥1024 毫克/升)。
在体外 UTI 模型中模拟,口服磷霉素治疗后,肺炎克雷伯菌尿分离株的再生长未得到充分抑制。高起始接种量进一步降低了疗效。