James Cook Drive, Rehabilitation Sciences Building, College of Healthcare Sciences, Sports and Exercise Science, James Cook University, Douglas, QLD, QLD481, Australia.
Sports Dynamix Private Limited, Chennai, India.
Sports Med. 2022 Jul;52(7):1623-1645. doi: 10.1007/s40279-022-01640-z. Epub 2022 Feb 26.
Several studies have examined the effect of creatine monohydrate (CrM) on indirect muscle damage markers and muscle performance, although pooled data from several studies indicate that the benefits of CrM on recovery dynamics are limited.
This systematic review and meta-analysis determined whether the ergogenic effects of CrM ameliorated markers of muscle damage and performance following muscle-damaging exercises.
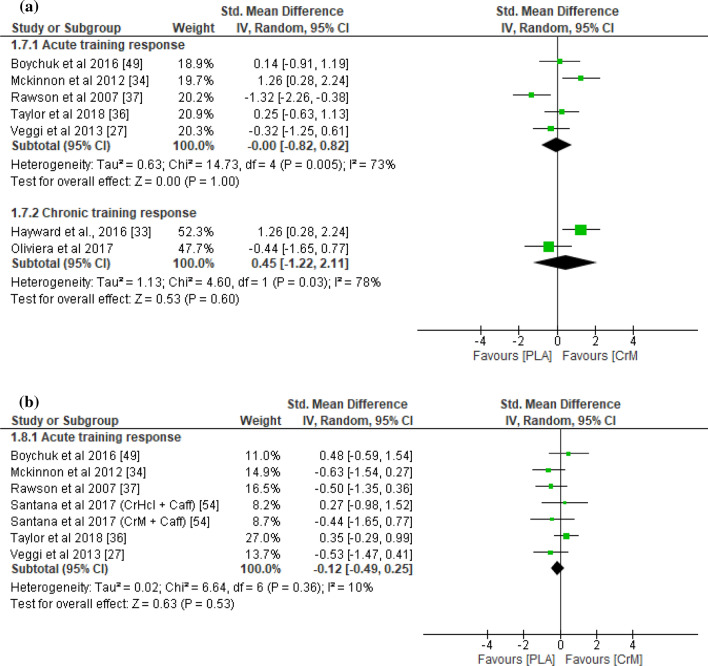
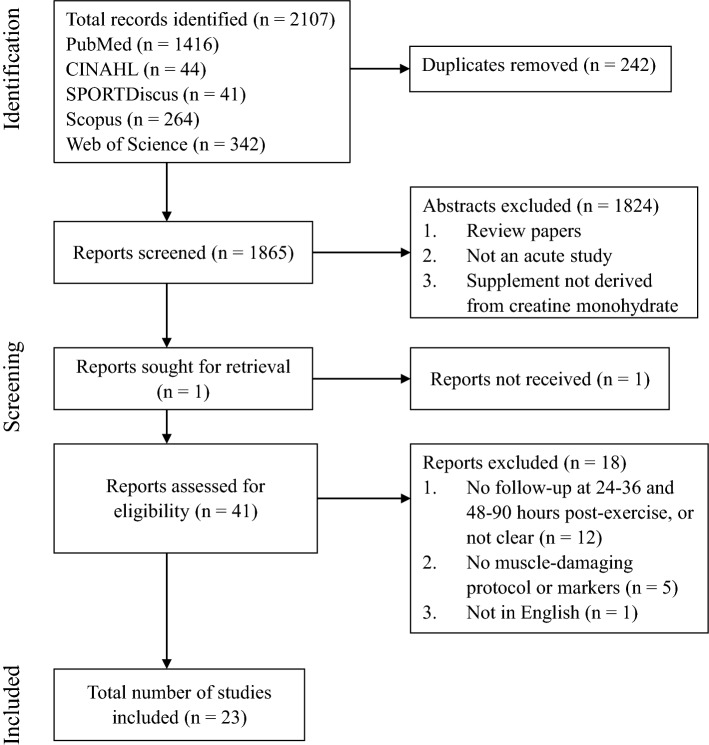
In total, 23 studies were included, consisting of 240 participants in the CrM group (age 23.9 ± 10.4 years, height 178 ± 5 cm, body mass 76.9 ± 7.6 kg, females 10.4%) and 229 participants in the placebo group (age 23.7 ± 8.5 years, height 177 ± 5 cm, body mass 77.0 ± 6.6 kg, females 10.0%). These studies were rated as fair to excellent following the PEDro scale. The outcome measures were compared between the CrM and placebo groups at 24-36 h and 48-90 h following muscle-damaging exercises, using standardised mean differences (SMDs) and associated p-values via forest plots. Furthermore, sub-group analyses were conducted by separating studies into those that examined the effects of CrM as an acute training response (i.e., after one muscle-damaging exercise bout) and those that examined the chronic training response (i.e., examining the acute response after the last training session following several weeks of training).
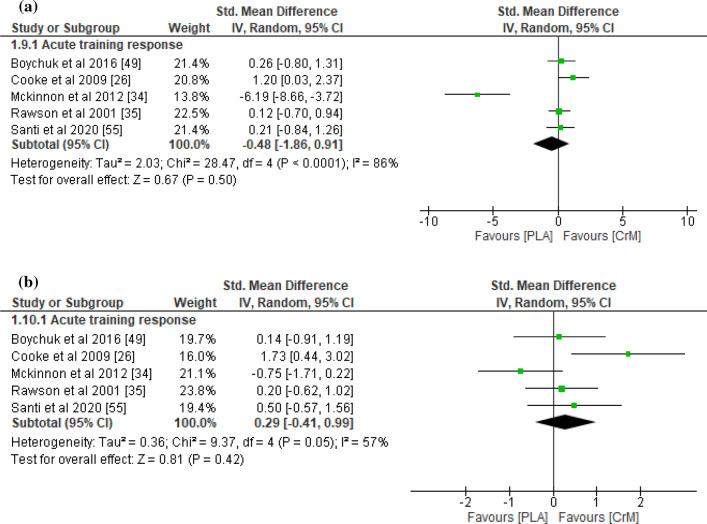
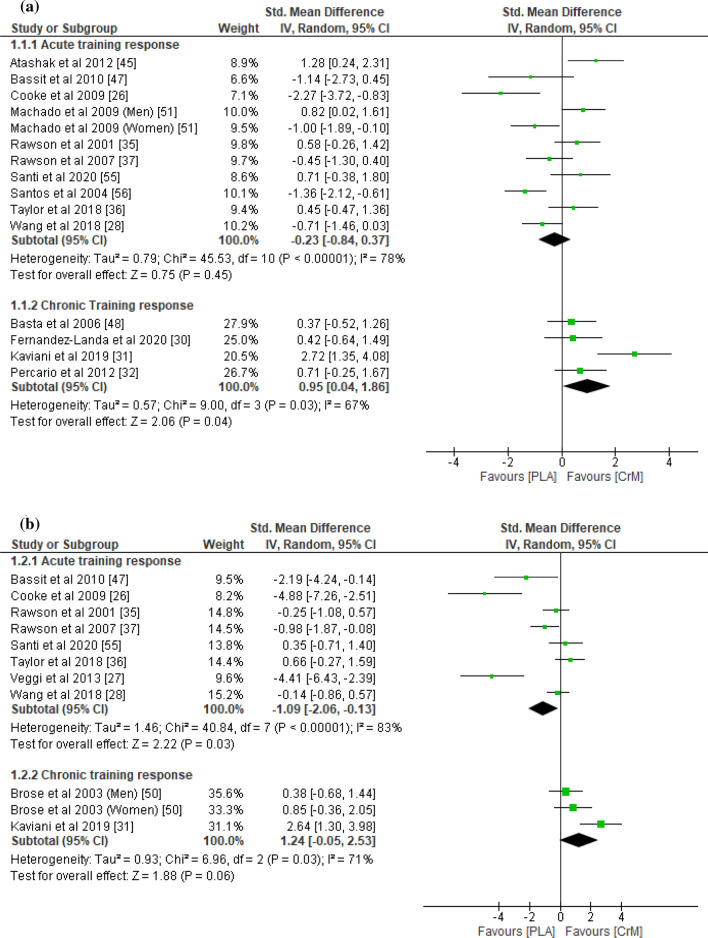
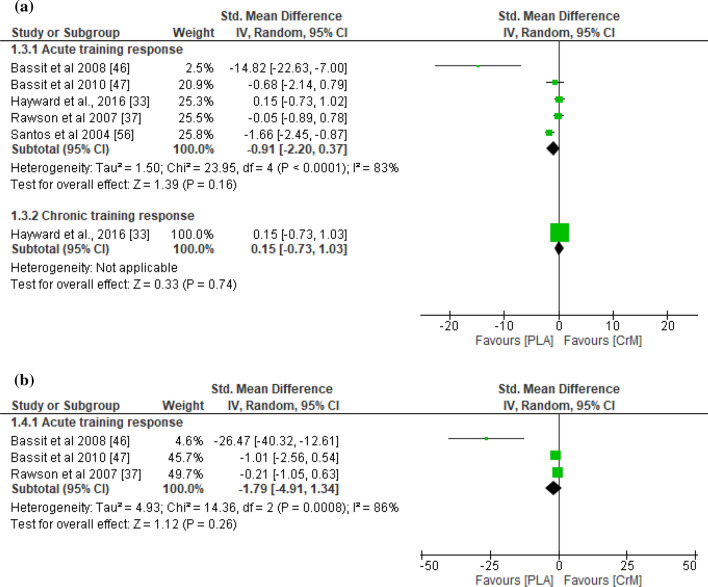
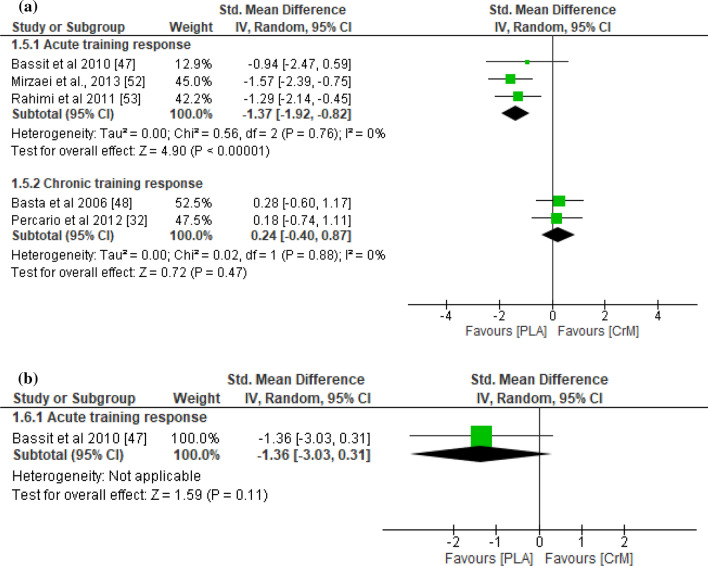
According to the meta-analysis, the CrM group exhibited significantly lower indirect muscle damage markers (i.e., creatine kinase, lactate dehydrogenase, and/or myoglobin) at 48-90 h post-exercise for the acute training response (SMD - 1.09; p = 0.03). However, indirect muscle damage markers were significantly greater in the CrM group at 24 h post-exercise (SMD 0.95; p = 0.04) for the chronic training response. Although not significant, a large difference in indirect muscle damage markers was also found at 48 h post-exercise (SMD 1.24) for the chronic training response. The CrM group also showed lower inflammation for the acute training response at 24-36 h post-exercise and 48-90 h post-exercise with a large effect size (SMD - 1.38 ≤ d ≤ - 1.79). Similarly, the oxidative stress markers were lower for the acute training response in the CrM group at 24-36 h post-exercise and 90 h post-exercise, with a large effect size (SMD - 1.37 and - 1.36, respectively). For delayed-onset muscle soreness (DOMS), the measures were lower for the CrM group at 24 h post-exercise with a moderate effect size (SMD - 0.66) as an acute training response. However, the inter-group differences for inflammation, oxidative stress, and DOMS were not statistically significant (p > 0.05).
Overall, our meta-analysis demonstrated a paradoxical effect of CrM supplementation post-exercise, where CrM appears to minimise exercise-induced muscle damage as an acute training response, although this trend is reversed as a chronic training response. Thus, CrM may be effective in reducing the level of exercise-induced muscle damage following a single bout of strenuous exercises, although training-induced stress could be exacerbated following long-term supplementation of CrM. Although long-term usage of CrM is known to enhance training adaptations, whether the increased level of exercise-induced muscle damage as a chronic training response may provide potential mechanisms to enhance chronic training adaptations with CrM supplementation remains to be confirmed.
已有多项研究探讨了肌酸单水合物(CrM)对间接肌肉损伤标志物和肌肉性能的影响,但几项研究的汇总数据表明,CrM 对恢复动态的益处有限。
本系统评价和荟萃分析旨在确定 CrM 的运动表现是否改善了肌肉损伤后的肌肉损伤标志物和性能。
共纳入 23 项研究,CrM 组 240 名参与者(年龄 23.9±10.4 岁,身高 178±5cm,体重 76.9±7.6kg,女性 10.4%),安慰剂组 229 名参与者(年龄 23.7±8.5 岁,身高 177±5cm,体重 77.0±6.6kg,女性 10.0%)。根据 PEDro 量表,这些研究的评分均为良好至优秀。使用标准均数差(SMD)和相关 p 值通过森林图比较 CrM 和安慰剂组在肌肉损伤后 24-36 小时和 48-90 小时的结果测量值。此外,还通过将研究分为急性训练反应(即一次肌肉损伤运动后)和慢性训练反应(即经过数周训练后的最后一次训练后急性反应)来进行亚组分析。
根据荟萃分析,在急性训练反应中,CrM 组在运动后 48-90 小时的间接肌肉损伤标志物(即肌酸激酶、乳酸脱氢酶和/或肌红蛋白)显著较低(SMD-1.09;p=0.03)。然而,在慢性训练反应中,CrM 组在运动后 24 小时的间接肌肉损伤标志物显著更高(SMD 0.95;p=0.04)。虽然不显著,但慢性训练反应中也发现间接肌肉损伤标志物在运动后 48 小时存在较大差异(SMD 1.24)。CrM 组在急性训练反应中也显示出较低的炎症标志物,在运动后 24-36 小时和 48-90 小时,具有较大的效应量(SMD-1.38≤d≤-1.79)。同样,在急性训练反应中,CrM 组在运动后 24-36 小时和 90 小时的氧化应激标志物也较低,具有较大的效应量(SMD-1.37 和-1.36)。对于延迟性肌肉酸痛(DOMS),CrM 组在运动后 24 小时的测量值较低,具有中等效应量(SMD-0.66)作为急性训练反应。然而,组间差异在炎症、氧化应激和 DOMS 方面无统计学意义(p>0.05)。
总的来说,我们的荟萃分析表明 CrM 补充后的运动表现存在矛盾效应,CrM 似乎作为急性训练反应最小化了运动引起的肌肉损伤,尽管这种趋势在慢性训练反应中逆转。因此,CrM 可能在减少单次剧烈运动后的运动诱导的肌肉损伤方面有效,尽管长期补充 CrM 可能会加剧训练引起的应激。尽管长期使用 CrM 已知可增强训练适应,但作为慢性训练反应的增加的运动诱导的肌肉损伤是否可能提供通过 CrM 补充增强慢性训练适应的潜在机制仍有待证实。