Hayashi Yuki, Nakase Hiroshi
Department of Gastroenterology and Hepatology, Sapporo Medical University of Medicine, Sapporo, Japan.
Front Physiol. 2022 Feb 11;13:845078. doi: 10.3389/fphys.2022.845078. eCollection 2022.
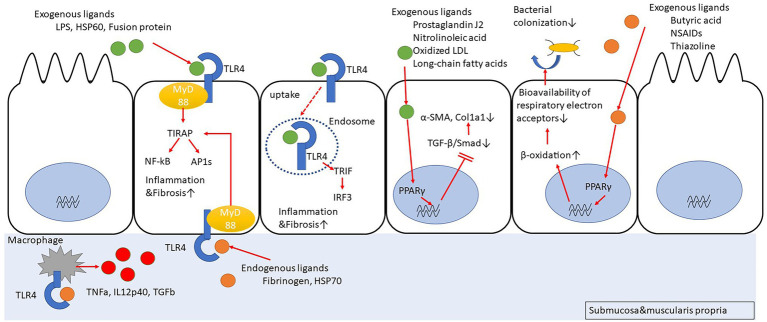
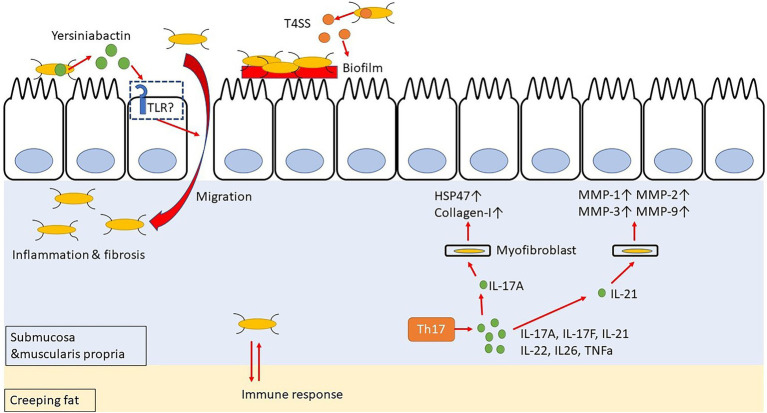
Crohn's disease (CD) is an inflammatory bowel disease (IBD) with repeated remissions and relapses. As the disease progresses, fibrosis and narrowing of the intestine occur, leading to severe complications such as intestinal obstruction. Endoscopic balloon dilatation, surgical stricture plasty, and bowel resection have been performed to treat intestinal stenosis. The clinical issue is that some patients with CD have a recurrence of intestinal stenosis even after the medical treatments. On the other hand, there exist no established medical therapies to prevent stenosis. With the progressive intestinal inflammation, cytokines and growth factors, including transforming growth factor (TGF-β), stimulate intestinal myofibroblasts, contributing to fibrosis of the intestine, smooth muscle hypertrophy, and mesenteric fat hypertrophy. Therefore, chronically sustained inflammation has long been considered a cause of intestinal fibrosis and stenosis. Still, even after the advent of biologics and tighter control of inflammation, intestinal fibrosis's surgical rate has not necessarily decreased. It is essential to elucidate the mechanisms involved in intestinal fibrosis in CD from a molecular biological level to overcome clinical issues. Recently, much attention has been paid to several key molecules of intestinal fibrosis: peroxisome proliferator-activating receptor gamma (PPARγ), toll-like receptor 4 (TLR4), adherent-invasive (AIEC), Th17 immune response, and plasminogen activator inhibitor 1 (PAI-1). As a major problem in the treatment of CD, the pathophysiology of patients with CD is not the same and varies depending on each patient. It is necessary to integrate these key molecules for a better understanding of the mechanism of intestinal inflammation and fibrosis.
克罗恩病(CD)是一种炎症性肠病(IBD),具有反复缓解和复发的特点。随着疾病进展,肠道会出现纤维化和狭窄,导致肠梗阻等严重并发症。内镜下球囊扩张、手术狭窄成形术和肠切除术已被用于治疗肠道狭窄。临床问题在于,一些CD患者即使经过治疗后仍会出现肠道狭窄复发。另一方面,目前尚无成熟的预防狭窄的药物治疗方法。随着肠道炎症的进展,包括转化生长因子(TGF-β)在内的细胞因子和生长因子会刺激肠道肌成纤维细胞,导致肠道纤维化、平滑肌肥大和肠系膜脂肪肥大。因此,长期持续的炎症一直被认为是肠道纤维化和狭窄的原因。然而,即使在生物制剂出现以及炎症得到更严格控制之后,肠道纤维化的手术率并不一定降低。从分子生物学层面阐明CD中肠道纤维化的相关机制对于解决临床问题至关重要。最近,肠道纤维化的几个关键分子受到了广泛关注:过氧化物酶体增殖物激活受体γ(PPARγ)、Toll样受体4(TLR4)、黏附侵袭性大肠杆菌(AIEC)、Th17免疫反应和纤溶酶原激活物抑制剂1(PAI-1)。作为CD治疗中的一个主要问题,CD患者的病理生理学各不相同,因患者而异。有必要整合这些关键分子,以更好地理解肠道炎症和纤维化的机制。