Department of Thoracic Surgery, Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, China.
Department of Laboratory Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Front Immunol. 2022 Feb 10;13:811007. doi: 10.3389/fimmu.2022.811007. eCollection 2022.
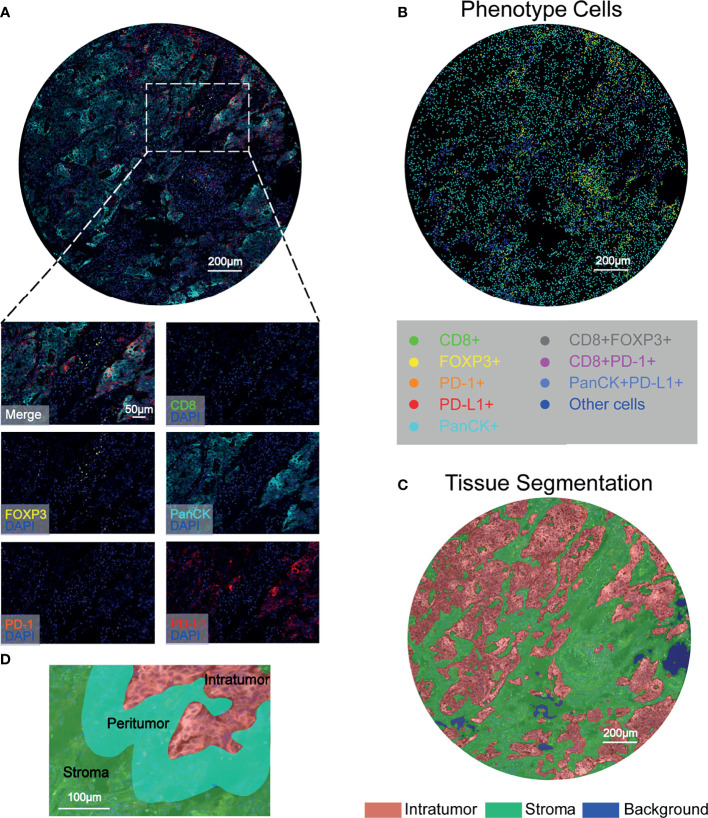
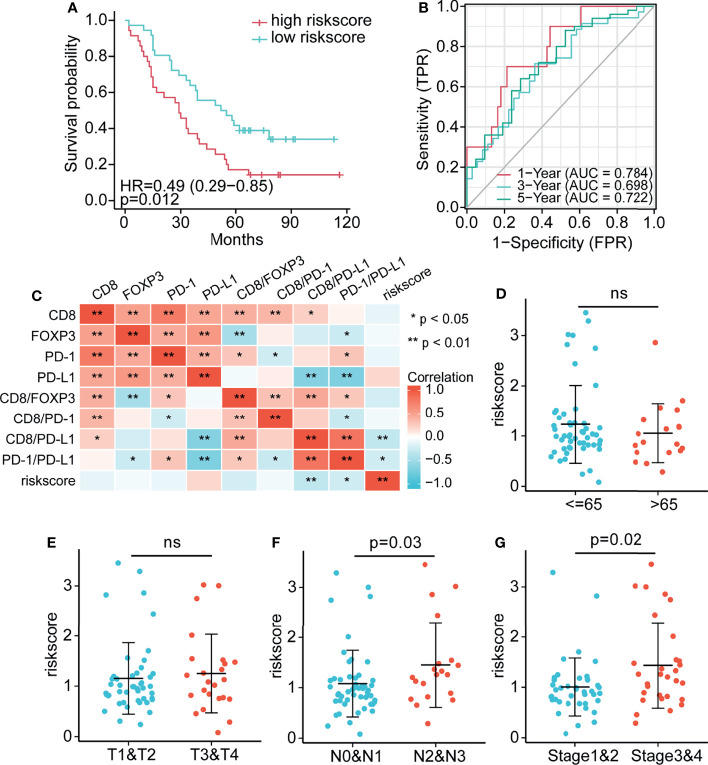
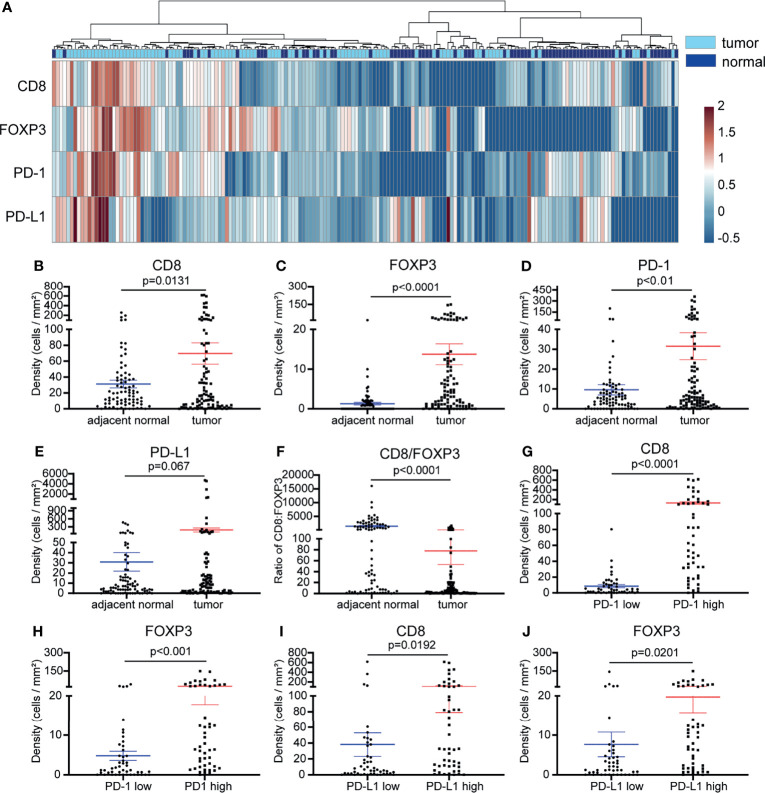
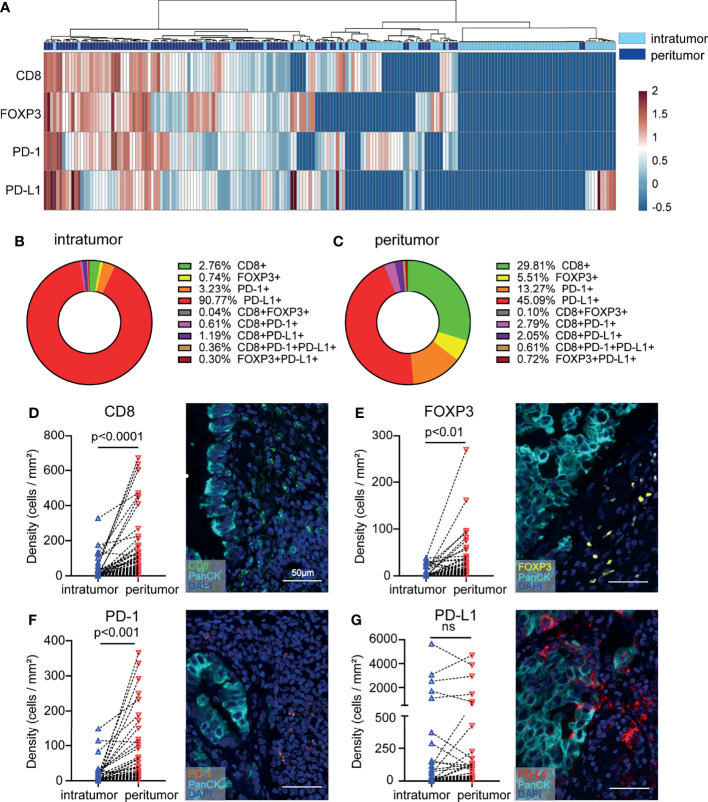
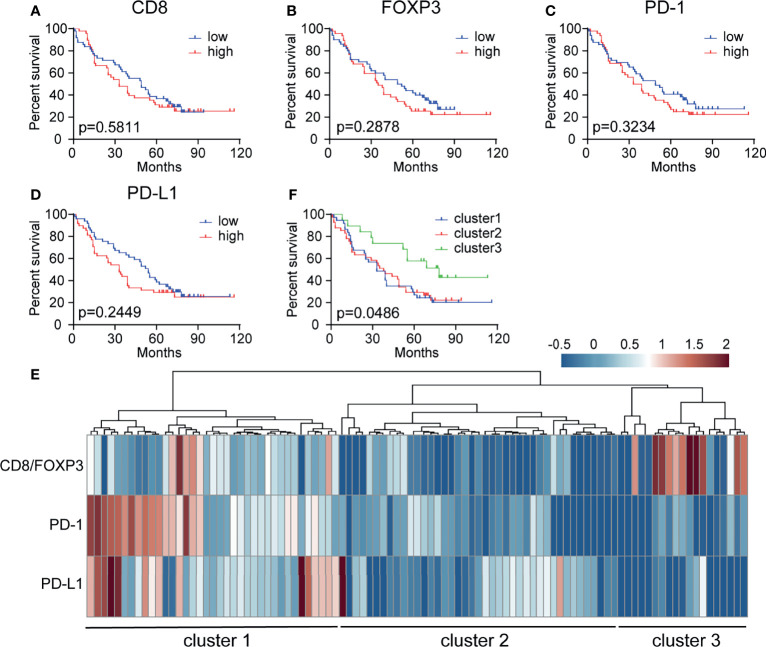
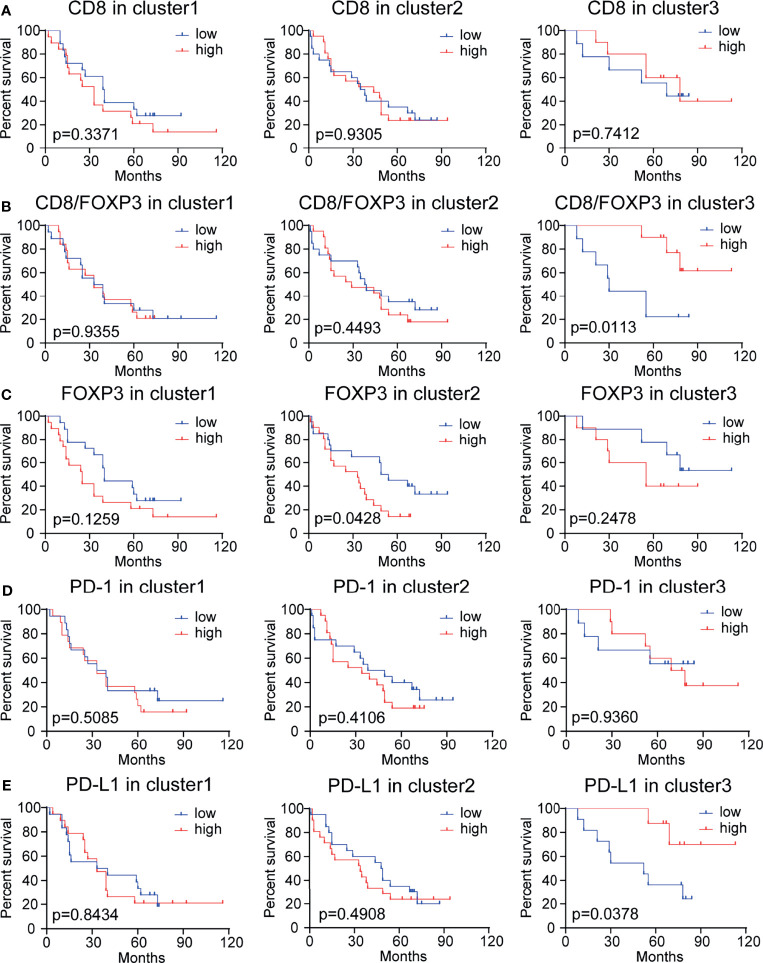
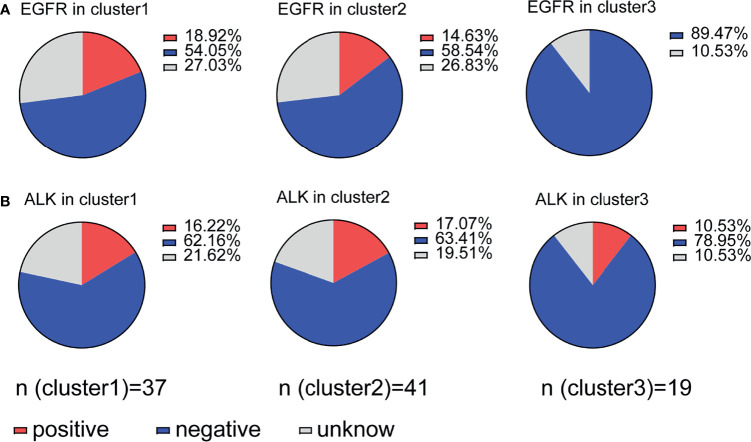
Given the complexity and highly heterogeneous nature of the microenvironment and its effects on antitumor immunity and cancer immune evasion, the prognostic value of a single immune marker is limited. Here, we show how the integration of immune checkpoint molecule expression and tumor-associated immune cell distribution patterns can influence prognosis prediction in non-small-cell lung cancer (NSCLC) patients. We analyzed tissue microarray (TMA) data derived from multiplex immunohistochemistry results and measured the densities of tumor-infiltrating CD8+ and FOXP3+ immune cells and tumor cells (PanCK+), as well as the densities of programmed cell death 1 (PD-1)+ and programmed cell death ligand 1 (PD-L1)+ cells in the peritumor and intratumor subregions. We found a higher density of infiltrating CD8+ and FOXP3+ immune cells in the peritumoral compartment than in the intratumoral compartment. In addition, unsupervised hierarchical clustering analysis of these markers revealed that the combination of high CD8/FOXP3 expression, low PD-1 and PD-L1 immune checkpoint expression, and lack of epidermal growth factor receptor (EGFR) mutation could be a favorable predictive marker. On the other hand, based on the clustering analysis, low CD8/FOXP3 and immune checkpoint (PD-1 and PD-L1) expression might be a marker for patients who are likely to respond to strategies targeting regulatory T (Treg) cells. Furthermore, an immune risk score model was established based on multivariate Cox regression, and the risk score was determined to be an independent prognostic factor for NSCLC patients. These results indicate that the immune context is heterogeneous because of the complex interactions of different components and that using multiple factors in combination might be promising for predicting the prognosis of and stratifying NSCLC patients.
鉴于肿瘤微环境的复杂性和高度异质性及其对抗肿瘤免疫和癌症免疫逃逸的影响,单一免疫标志物的预后价值有限。在这里,我们展示了如何整合免疫检查点分子表达和肿瘤相关免疫细胞分布模式来影响非小细胞肺癌(NSCLC)患者的预后预测。我们分析了来自多重免疫组化结果的组织微阵列(TMA)数据,并测量了肿瘤浸润性 CD8+和 FOXP3+免疫细胞以及肿瘤细胞(PanCK+)的密度,以及肿瘤周围和肿瘤内亚区 PD-1+和 PD-L1+细胞的密度。我们发现肿瘤周围区的浸润性 CD8+和 FOXP3+免疫细胞密度高于肿瘤内区。此外,对这些标志物的无监督层次聚类分析显示,高 CD8/FOXP3 表达、低 PD-1 和 PD-L1 免疫检查点表达以及缺乏表皮生长因子受体(EGFR)突变的组合可能是一个有利的预测标志物。另一方面,基于聚类分析,低 CD8/FOXP3 和免疫检查点(PD-1 和 PD-L1)表达可能是对靶向调节性 T(Treg)细胞的策略可能有反应的患者的标志物。此外,还基于多变量 Cox 回归建立了免疫风险评分模型,风险评分被确定为 NSCLC 患者的独立预后因素。这些结果表明,由于不同成分的复杂相互作用,免疫背景具有异质性,并且联合使用多种因素可能是预测 NSCLC 患者预后和分层的有前途的方法。