MRC Integrative Epidemiology Unit at the University of Bristol, Bristol, UK.
NIHR Bristol Biomedical Research Centre, University of Bristol, Bristol, UK.
BMC Med. 2020 Nov 23;18(1):366. doi: 10.1186/s12916-020-01819-z.
Prediction of pregnancy-related disorders is usually done based on established and easily measured risk factors. Recent advances in metabolomics may provide earlier and more accurate prediction of women at risk of pregnancy-related disorders.
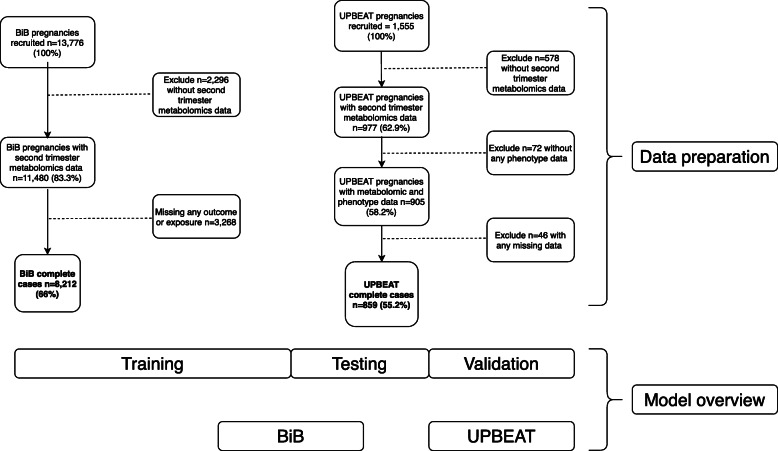
We used data collected from women in the Born in Bradford (BiB; n = 8212) and UK Pregnancies Better Eating and Activity Trial (UPBEAT; n = 859) studies to create and validate prediction models for pregnancy-related disorders. These were gestational diabetes mellitus (GDM), hypertensive disorders of pregnancy (HDP), small for gestational age (SGA), large for gestational age (LGA) and preterm birth (PTB). We used ten-fold cross-validation and penalised regression to create prediction models. We compared the predictive performance of (1) risk factors (maternal age, pregnancy smoking, body mass index (BMI), ethnicity and parity) to (2) nuclear magnetic resonance-derived metabolites (N = 156 quantified metabolites, collected at 24-28 weeks gestation) and (3) combined risk factors and metabolites. The multi-ethnic BiB cohort was used for training and testing the models, with independent validation conducted in UPBEAT, a multi-ethnic study of obese pregnant women.
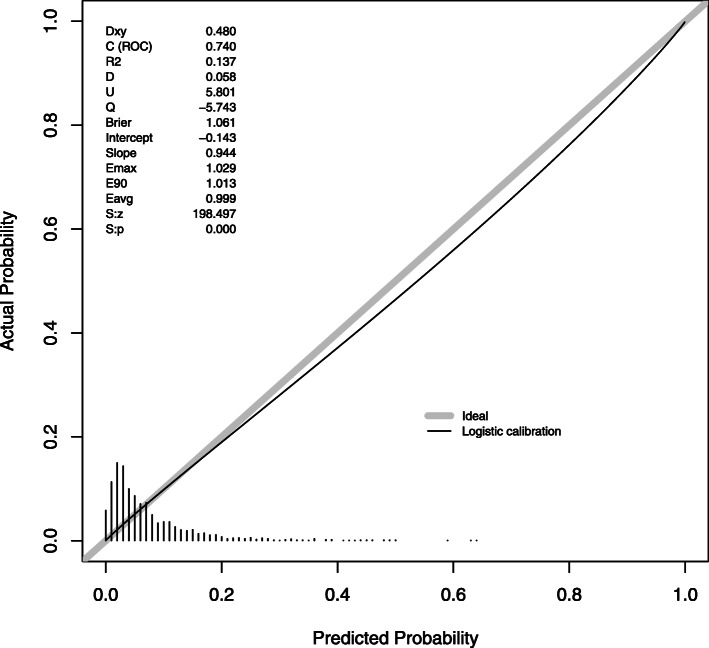
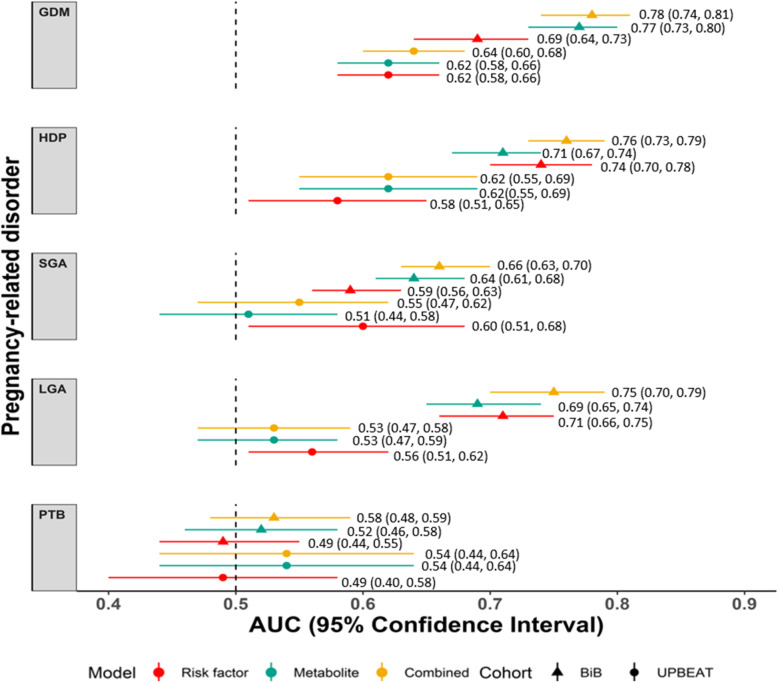
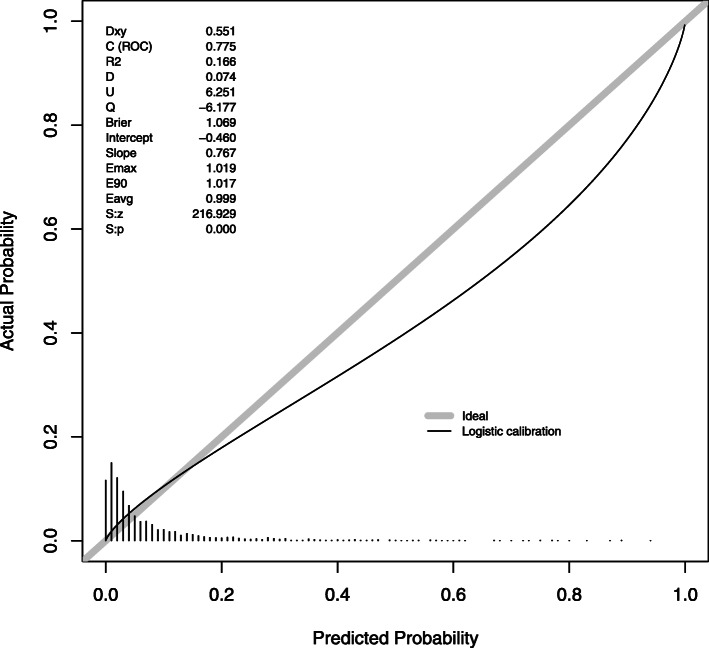
Maternal age, pregnancy smoking, BMI, ethnicity and parity were retained in the combined risk factor and metabolite models for all outcomes apart from PTB, which did not include maternal age. In addition, 147, 33, 96, 51 and 14 of the 156 metabolite traits were retained in the combined risk factor and metabolite model for GDM, HDP, SGA, LGA and PTB, respectively. These include cholesterol and triglycerides in very low-density lipoproteins (VLDL) in the models predicting GDM, HDP, SGA and LGA, and monounsaturated fatty acids (MUFA), ratios of MUFA to omega 3 fatty acids and total fatty acids, and a ratio of apolipoprotein B to apolipoprotein A-1 (APOA:APOB1) were retained predictors for GDM and LGA. In BiB, discrimination for GDM, HDP, LGA and SGA was improved in the combined risk factors and metabolites models. Risk factor area under the curve (AUC 95% confidence interval (CI)): GDM (0.69 (0.64, 0.73)), HDP (0.74 (0.70, 0.78)) and LGA (0.71 (0.66, 0.75)), and SGA (0.59 (0.56, 0.63)). Combined risk factor and metabolite models AUC 95% (CI): GDM (0.78 (0.74, 0.81)), HDP (0.76 (0.73, 0.79)) and LGA (0.75 (0.70, 0.79)), and SGA (0.66 (0.63, 0.70)). For GDM, HDP and LGA, but not SGA, calibration was good for a combined risk factor and metabolite model. Prediction of PTB was poor for all models. Independent validation in UPBEAT at 24-28 weeks and 15-18 weeks gestation confirmed similar patterns of results, but AUCs were attenuated.
Our results suggest a combined risk factor and metabolite model improves prediction of GDM, HDP and LGA, and SGA, when compared to risk factors alone. They also highlight the difficulty of predicting PTB, with all models performing poorly.
妊娠相关疾病的预测通常基于已建立且易于测量的风险因素。代谢组学的最新进展可能为妊娠相关疾病风险的女性提供更早、更准确的预测。
我们使用来自 Born in Bradford (BiB; n = 8212) 和 UK Pregnancies Better Eating and Activity Trial (UPBEAT; n = 859) 研究的女性数据,创建并验证了与妊娠相关疾病相关的预测模型。这些疾病包括妊娠糖尿病 (GDM)、妊娠高血压疾病 (HDP)、胎儿生长受限 (SGA)、胎儿生长过大 (LGA) 和早产 (PTB)。我们使用十折交叉验证和惩罚回归来创建预测模型。我们比较了(1)风险因素(母亲年龄、妊娠吸烟、体重指数 (BMI)、种族和产次)与(2)基于核磁共振的代谢物(在 24-28 周妊娠时采集的 156 种定量代谢物)和(3)风险因素和代谢物的组合,预测这些疾病的表现。多民族 BiB 队列用于训练和测试模型,在 UPBEAT 中进行了独立验证,这是一项针对肥胖孕妇的多民族研究。
除了不包括母亲年龄的 PTB 外,母亲年龄、妊娠吸烟、BMI、种族和产次在所有结局的综合风险因素和代谢物模型中都得到了保留。此外,在 GDM、HDP、SGA、LGA 和 PTB 的综合风险因素和代谢物模型中,156 种代谢物特征中有 147、33、96、51 和 14 种分别保留。这些包括预测 GDM、HDP、SGA 和 LGA 的极低密度脂蛋白 (VLDL) 中的胆固醇和甘油三酯,以及预测 GDM 和 LGA 的单不饱和脂肪酸 (MUFA)、MUFA 与 omega 3 脂肪酸的比值和总脂肪酸以及载脂蛋白 B 与载脂蛋白 A-1 (APOA:APOB1) 的比值。在 BiB 中,综合风险因素和代谢物模型提高了 GDM、HDP、LGA 和 SGA 的鉴别能力。风险因素曲线下面积(95%置信区间(CI)):GDM(0.69(0.64,0.73))、HDP(0.74(0.70,0.78))和 LGA(0.71(0.66,0.75)),以及 SGA(0.59(0.56,0.63))。综合风险因素和代谢物模型 AUC 95%(CI):GDM(0.78(0.74,0.81))、HDP(0.76(0.73,0.79))和 LGA(0.75(0.70,0.79)),以及 SGA(0.66(0.63,0.70))。对于 GDM、HDP 和 LGA,但不是 SGA,综合风险因素和代谢物模型的校准效果良好。所有模型对 PTB 的预测均较差。在 24-28 周和 15-18 周妊娠时在 UPBEAT 中的独立验证证实了类似的结果模式,但 AUC 减弱。
我们的研究结果表明,与单独使用风险因素相比,综合风险因素和代谢物模型可以改善 GDM、HDP 和 LGA 以及 SGA 的预测。它们还突出了预测 PTB 的困难,所有模型的表现都很差。