From the Department of Radiology (R.P., J.A.A., P.G., M.S.G.), Druckenmiller Center for Lung Cancer Research (R.P., K.S.T., N.R., M.S.G., D.R.J.), Thoracic Surgery Service (J.G.C., R.C., J.Z., D.R.J.), Biostatistics Service, Department of Epidemiology and Biostatistics (K.W., K.S.T.), and Department of Pathology (N.R.), Memorial Sloan Kettering Cancer Center, 1275 York Ave, Box 7, New York, NY 10065.
Radiology. 2022 Jun;303(3):664-672. doi: 10.1148/radiol.211582. Epub 2022 Mar 1.
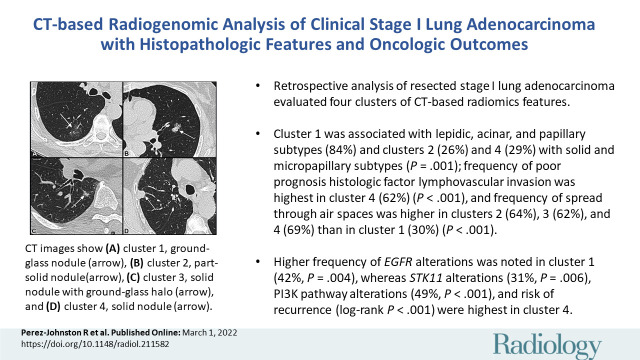
Background A preoperative predictive model is needed that can be used to identify patients with lung adenocarcinoma (LUAD) who have a higher risk of recurrence or metastasis. Purpose To investigate associations between CT-based radiomic consensus clustering of stage I LUAD and clinical-pathologic features, genomic data, and patient outcomes. Materials and Methods Patients who underwent complete surgical resection for LUAD from April 2014 to December 2017 with preoperative CT and next-generation sequencing data were retrospectively identified. Comprehensive radiomic analysis was performed on preoperative CT images; tumors were classified as solid, ground glass, or mixed. Patients were clustered into groups based on their radiomics features using consensus clustering, and clusters were compared with tumor genomic alterations, histopathologic features, and recurrence-specific survival (Kruskal-Wallis test for continuous data, χ or Fisher exact test for categorical data, and log-rank test for recurrence-specific survival). Cluster analysis was performed on the entire cohort and on the solid, ground-glass, and mixed lesion subgroups. Results In total, 219 patients were included in the study (median age, 68 years; interquartile range, 63-74 years; 150 [68%] women). Four radiomic clusters were identified. Cluster 1 was associated with lepidic, acinar, and papillary subtypes (76 of 90 [84%]); clusters 2 (13 of 50 [26%]) and 4 (13 of 45 [29%]) were associated with solid and micropapillary subtypes ( < .001). The alterations were highest in cluster 1 (38 of 90 [42%], = .004). Clusters 2, 3, and 4 were associated with lymphovascular invasion (19 of 50 [38%], 14 of 34 [41%], and 28 of 45 [62%], respectively; < .001) and tumor spread through air spaces (32 of 50 [64%], 21 of 34 [62%], and 31 of 45 [69%], respectively; < .001). alterations (14 of 45 [31%]; = .006), phosphoinositide 3-kinase pathway alterations (22 of 45 [49%], < .001), and risk of recurrence (log-rank < .001) were highest in cluster 4. Conclusion CT-based radiomic consensus clustering enabled identification of associations between radiomic features and clinicalpathologic and genomic features and outcomes in patients with clinical stage I lung adenocarcinoma. © RSNA, 2022 See also the editorial by Nishino in this issue.
背景 需要一种术前预测模型,用于识别肺腺癌(LUAD)患者,这些患者具有更高的复发或转移风险。目的 探讨 CT 基于放射组学共识聚类的 I 期 LUAD 与临床病理特征、基因组数据和患者结局之间的关联。材料与方法 回顾性分析 2014 年 4 月至 2017 年 12 月期间因 LUAD 行完全手术切除且术前有 CT 和下一代测序数据的患者。对术前 CT 图像进行全面的放射组学分析;肿瘤分为实性、磨玻璃样或混合性。根据放射组学特征对患者进行共识聚类分组,并对聚类与肿瘤基因组改变、组织病理学特征和复发特异性生存进行比较(连续数据的 Kruskal-Wallis 检验、分类数据的 χ 检验或 Fisher 确切检验、以及复发特异性生存的对数秩检验)。对整个队列和实性、磨玻璃样和混合性病变亚组进行聚类分析。结果 共纳入 219 例患者(中位年龄,68 岁;四分位间距,63-74 岁;150 [68%] 例女性)。确定了 4 个放射组学聚类。聚类 1 与贴壁、腺泡和乳头亚型相关(76/90 [84%]);聚类 2(50/50 [26%])和聚类 4(45/45 [29%])与实性和微乳头亚型相关( <.001)。聚类 1 的 改变率最高(38/90 [42%], =.004)。聚类 2、3 和 4 与脉管侵犯(50/50 [64%]、34/34 [41%]和 45/45 [62%], <.001)和肿瘤通过气腔播散(50/50 [64%]、34/34 [62%]和 45/45 [69%], <.001)相关。聚类 4 的 改变率(14/45 [31%]; =.006)、磷酸肌醇 3-激酶通路改变率(22/45 [49%], <.001)和复发风险(对数秩 <.001)最高。结论 CT 基于放射组学的共识聚类可识别临床 I 期肺腺癌患者的放射组学特征与临床病理和基因组特征及结局之间的关联。