Department of Surgery, Selkirk Regional Health Centre, 120 Easton Drive, Selkirk, MB, R1A 2M2, Canada.
Easton Place Clinic, Box 400, 15 Wersch Street, Selkirk, MB, R1A 2B3, Canada.
BMC Gastroenterol. 2022 Mar 3;22(1):95. doi: 10.1186/s12876-022-02161-9.
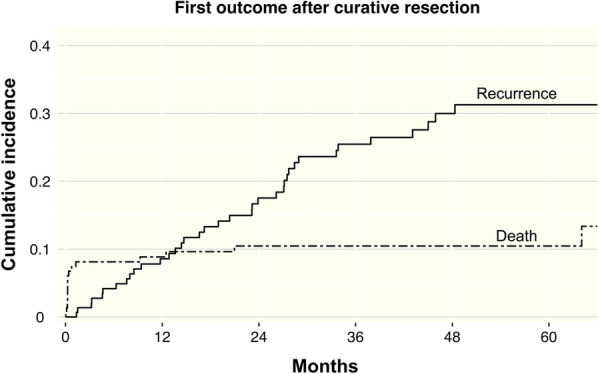
This study examines the effect of prognostic patient and disease characteristics on colorectal cancer (CRC) recurrence after curative resection. We used competing risk analysis with death as a competing risk. This method provides the clinician a perspective into a patient's actual risk of experiencing a recurrence.
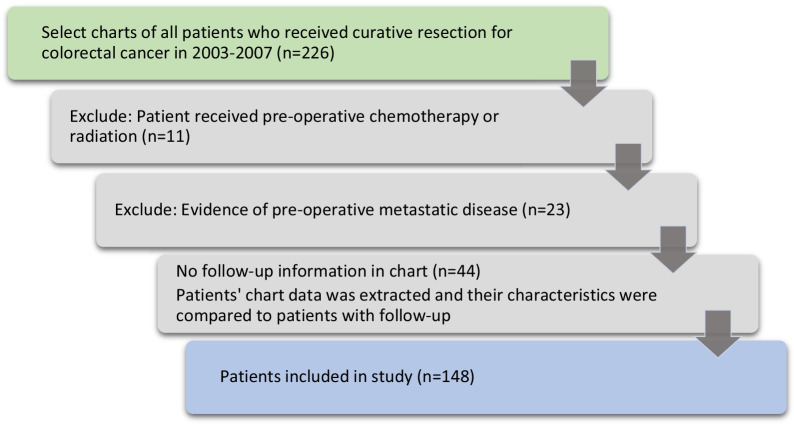
A retrospective cohort study of patients diagnosed with CRC who underwent curative resection for CRC from 2003-2007 at the Royal University Hospital in Saskatoon was completed. The outcome of interest was the first CRC recurrence, either local or distant metastasis. Demographic data, tumor characteristics, adjuvant treatment and follow-up data, date of local recurrence or metastasis were recorded from the medical record. Univariate analysis was completed to look at the relationship between each of the prognostic indicators and recurrence. Multivariable modelling (subdistribution regression modelling) was done to identify the main risk factors in determining recurrence.
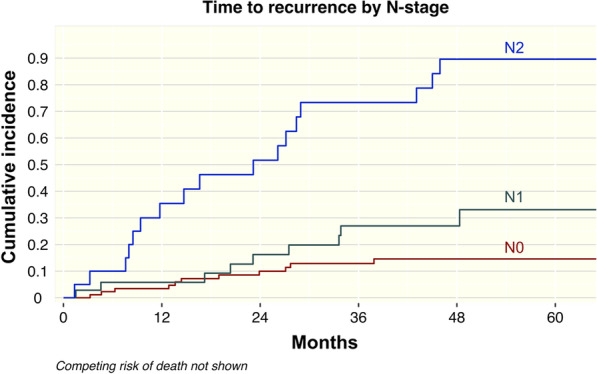
Of 148 patients, 38 (25.7%) experienced a recurrence, 16 (10.8%) died without evidence of recurrence, and 94 (63.5%) experienced neither outcome. The median follow-up was 30.5 months (interquartile range 10.6-50). In univariable subdistribution regression, T-stage, N-stage, vascular invasion and positive margins were all predictive of cancer recurrence, with p ≤ 0.001, with subdistribution hazard ratios for T4 stage at 11.93, T3 stage at 2.46, N2 stage at 10.58, and presence of vascular invasion at 4.27. N-stage remained as the sole predictor in multivariable regression. Cumulative incidence function (CIF) of recurrence at 48 months after surgery was 15%, 27% and 90% for N1/2, N3 and N4 respectively.
The highest CIF of recurrence was associated with T4 stage, N2 stage, and vascular invasion. Patient's age, tumour location, type, or histological grade were not found to have a significant effect on the success of CRC surgery in precluding a recurrence.
本研究旨在探讨预后患者和疾病特征对结直肠癌(CRC)根治性切除术后复发的影响。我们使用竞争风险分析,以死亡为竞争风险。这种方法为临床医生提供了一个视角,了解患者实际复发的风险。
对 2003 年至 2007 年期间在萨斯卡通皇家大学医院接受 CRC 根治性切除术的 CRC 患者进行了回顾性队列研究。感兴趣的结局是首次 CRC 复发,无论是局部复发还是远处转移。从病历中记录人口统计学数据、肿瘤特征、辅助治疗和随访数据、局部复发或转移的日期。完成单变量分析以研究每个预后指标与复发之间的关系。多变量建模(亚分布回归建模)用于确定决定复发的主要危险因素。
在 148 名患者中,38 名(25.7%)发生了复发,16 名(10.8%)死于无复发证据,94 名(63.5%)未发生这两种结局。中位随访时间为 30.5 个月(四分位距 10.6-50)。在单变量亚分布回归中,T 分期、N 分期、血管侵犯和阳性切缘均与癌症复发相关,p≤0.001,T4 期的亚分布危险比为 11.93,T3 期为 2.46,N2 期为 10.58,血管侵犯为 4.27。多变量回归中,N 分期仍然是唯一的预测因素。术后 48 个月时的复发累积发生率(CIF)分别为 N1/2、N3 和 N4 为 15%、27%和 90%。
复发的最高 CIF 与 T4 期、N2 期和血管侵犯有关。患者的年龄、肿瘤位置、类型或组织学分级与 CRC 手术成功无关,不会增加复发的风险。